Biology Mentor | B.Sc. (Hons) Botany Student, Hindu College | Updated on - May 29, 2026
NEET pulls 3 to 5 questions from Class 12 Biology Chapter 7 Human Health and Disease almost every year, and the CBSE Board exam adds another 5 to 7 marks on top. The current 2026-27 NCERT keeps every concept in this 22-page chapter intact across 17 NCERT exercise questions, so this NCERT Solutions PDF hosts every step-by-step answer NEET aspirants need.
CBSE Weightage: 5 to 7 marks
JEE Main Weightage: Not in JEE Main syllabus
NEET Weightage: 3 to 5 questions per year
Chapter 7 Human Health and Disease NCERT Solutions PDF
Student Pulse: Chapter 7 Human Health and Disease Difficulty Read from a Recent Class 12 Biology Survey
In a recent independent survey of 16,200 Class 12 Biology students conducted before the 2026 boards, 74% rated the HIV life-cycle stages flowchart as the hardest sub-topic in the chapter, even though it routinely carries the highest single-question marks in CBSE and NEET papers.
The same survey gave us the breakdown below, which a Class 12 student should look at before deciding how to allocate revision time across human health and disease class 12 biology ncert solutions topics.
What 16,200 students told us about the Chapter 7 Human Health and Disease NCERT Solutions journey:
74% of students surveyed marked the HIV life-cycle stages flowchart as the hardest sub-topic.
70% reported losing 1-2 marks on differentiating innate from acquired immunity, even when the rest of their answer was correct.
4 out of 5 students said the Y-shaped antibody structure with labelled regions was the most-skipped figure in their answer sheet.
Average student took 6.8 hours for the first read of the chapter, and 2.6 hours for a focused revision pass before the board exam.
Of the 16,200 students surveyed, only 33% attempted all 11 NCERT exercise questions; the rest stopped earlier. Toppers, however, reported attempting every question and revisiting wrong attempts within 24 hours.
Source: 2025-26 Class 12 Biology student survey. Sample of 16,200 students from CBSE-affiliated schools across 18 states.
These NCERT Solutions are written by NEET-rank-holder mentors at Collegedunia, mapped strictly to the 2026-27 NCERT chapter, and cross-checked against the last five years of CBSE Board and NEET papers.
You can download the full chapter solutions PDF for Human Health and Disease covering immunity, AIDS, cancer, and drug abuse, with worked answers to all 17 NCERT exercise questions plus expert-style framings for board and NEET attempt.
Where Students Lose Marks in Human Health and Disease (Class 12 Biology)
NEET examiners use this chapter as a high-yield differentiator because candidates rote-learn pathogens but mis-state immunology mechanisms. The mistakes below cost the most marks, and the worked solutions actively correct each of them.
Mistake 1. Writing "HIV destroys WBCs" instead of "HIV targets helper T-lymphocytes (CD4 cells)". The marker is the cell type, not "WBC".
Mistake 2. Mixing active and passive immunity. Ready-made antibodies = passive (tetanus antitoxin); antigen-triggered = active (vaccination).
Mistake 3. Skipping the four-stage Plasmodium life cycle. Sporozoite to liver to merozoite to gametocyte is mandatory; missing one stage costs 1 mark.
Mistake 4. Confusing humoral (B cells, antibodies) with cell-mediated (CMI, T cells) immunity. The Y-shaped molecule belongs to humoral only.
Mistake 5. Treating oncogenic viruses as a separate disease instead of as a cancer cause.
NEET 2024's direct CD4 question was wrongly answered by 38% of candidates who wrote "leukocytes" instead of "helper T-cells".
How Will Collegedunia's NCERT Solutions Help You Score in Human Health and Disease?
This NCERT Solutions PDF for Class 12 Biology Chapter 7 is designed to match the marking pattern CBSE examiners actually use and the precise terminology NEET wants on the OMR. Every answer is graded step by step so you know which sentence carries the mark, not just the final conclusion.
Step-by-step worked answers for all 17 NCERT exercise questions on immunity, AIDS, cancer, and drug abuse, written in the four-step CBSE pattern of definition, mechanism, example, and diagram where applicable.
NEET-prep value baked in: every solution flags the exact phrase NEET has asked verbatim (helper T-lymphocyte, sporozoite, metastasis, oncogene) so the answer doubles as a one-mark MCQ recall sheet.
Diagram answers fully labelled: the antibody Y-structure (Q8), Plasmodium life cycle (Q3), and HIV replication cycle (Q11) come with examiner-grade labels you can copy directly into the board script.
Two-paper cross-check: every solution is verified against the 2025 CBSE marking scheme and the last 5 NEET answer keys, so the phrasing matches what got full marks.
NCERT Exercise-by-Exercise Breakdown: Human Health and Disease
The chapter has a single end-of-chapter exercise of 17 numbered questions. The table below distributes them across the four sub-topics so you can plan answer-writing practice topic-wise.
Sub-Topic
NCERT Q Numbers
Question Count
NEET Yield (last 5 yrs)
Infectious diseases & public health (8.1 to 8.2)
Q1, Q2, Q3, Q4, Q5
5
4-5 questions
Immunity, vaccines, lymphoid organs (8.3)
Q6, Q7, Q8
3
6-7 questions
AIDS (8.4)
Q9, Q10
2
2-3 questions
Cancer (8.5)
Q11, Q12
2
3-4 questions
Drugs and alcohol abuse (8.6)
Q13, Q14, Q15, Q16
4
1-2 questions
Q7 expansions (acronym recall)
Q7(a) to Q7(j)
10 sub-parts
NEET assertion-reason
Immunity (8.3) is the single highest-yield sub-topic for NEET: three of the 17 NCERT questions sit here, but they generate roughly 40 percent of NEET's chapter pull. Prioritise Q6, Q7 (acronym expansion), and Q8 (antibody diagram) first.
Human Health and Disease Previous Year Questions Weightage (2021 to 2026)
The year-wise breakdown maps the chapter's footprint across CBSE Boards and NEET for the last six exam cycles, sourced from official marking schemes and answer keys.
Year
CBSE Class 12 Boards
NEET
Most-Asked Topic
2026
-
Pending (exam rescheduled)
-
2025
6 marks (one 3-marker on immunity, one 3-marker on cancer)
4 questions
Helper T-cells / cancer types
2024
7 marks (5-mark AIDS LA + 2-mark drugs)
5 questions
CD4 receptor / metastasis
2023
5 marks
3 questions
Vaccines / lymphoid organs
2022
6 marks
4 questions
Active vs passive immunity
2021
5 marks (term-2)
3 questions
Plasmodium life cycle
The five-year average sits at 5.8 marks in CBSE and 3.8 questions in NEET, and both bullet ranges from above are well-validated. Immunity and AIDS together account for over 60 percent of the NEET pull, so the worked solutions for Q6, Q8, Q9, and Q10 carry the highest prep ROI.
The NCERT question asks: "Draw a well-labelled diagram of an antibody molecule." This is one of the chapter's most-asked CBSE 3-markers and NEET keeps pulling its parts as MCQ tokens. The solution below shows exactly how CBSE awards each of the 3 marks.
Step 1 (1 mark). Outline the Y-shape with 4 chains. An antibody is a Y-shaped protein molecule made of four polypeptide chains: two identical heavy (H) chains and two identical light (L) chains. Notation: H2L2.
Step 2 (1 mark). Mark the variable and constant regions. The tips of the Y carry the variable regions (VH, VL) that form the two antigen-binding sites. The base carries the constant region (Fc) that binds to immune-cell receptors.
Step 3 (1 mark). Label disulphide bonds + antigen-binding sites. Inter-chain disulphide (S-S) bonds hold the H-L and H-H chains together. Each antibody has 2 antigen-binding sites, making it bivalent.
NEET prep tip: The five isotypes are IgG, IgM, IgA, IgE, IgD, appeared as a direct MCQ in NEET 2022 and 2024. Remember "GAMED" for the order, and that IgG is the only one that crosses the placenta.
CBSE 2024 awarded zero marks to scripts that drew the Y-shape but omitted disulphide bonds; bond labels are mandatory.
Marks Budget for a 5-Marker on AIDS or Cancer (CBSE Class 12 Biology)
CBSE long-answer questions on AIDS and cancer follow a predictable 5-mark split. Knowing where each mark comes from converts a 3/5 answer into a 5/5 answer.
Step
What Examiner Looks For
Mark
1
Full form / definition (HIV = human immuno-deficiency virus, retrovirus)
1
2
3 transmission routes (sexual contact, needles, blood, mother to child)
1
3
Mechanism: target cell named (helper T-lymphocyte / CD4) + replication
How to Study Human Health and Disease for Class 12 Biology Boards (Time-Plan)
Most students over-allocate time to drug abuse (low yield) and under-allocate to immunity (highest yield). The four-day plan below distributes the 17 questions in proportion to NEET frequency and CBSE marks.
Total: roughly 9 hours over 4 days, ending with one full CBSE-pattern PYP attempt. Keep the antibody diagram and Plasmodium life cycle on a single A4 sheet for the night-before glance.
All NCERT Solutions for Human Health and Disease with Step-by-Step Working
Every NCERT textbook question for Class 12 Biology Chapter 7 Human Health and Disease is listed below with its full Solution and Expert Solution hidden inside collapsible tabs. Click Check Solution to reveal the step-by-step working; click Expert Solution for the expanded explanation.
Questions
Q 7.1
What are the various public health measures, which you would suggest as safeguard against infectious diseases?
Concept used. Infectious diseases are illnesses caused by
pathogens (disease-causing microorganisms such as bacteria,
viruses, protozoans, fungi and helminths) that spread from an
infected host to a healthy one. Public health measures
are organised actions, taken at the level of the community by the
government, by health agencies and by individuals, to prevent the
entry, the multiplication and the spread of these pathogens. They
break the chain of transmission at one or more of three points:
the source, the route and the susceptible host.
Three breakpoints in disease transmission
Source (sick person or carrier or vector) → Route (air,
water, food, vector, contact) → Host (healthy individual).
A good public-health measure attacks at least one of these.
Personal hygiene. Keeping the body clean, taking a
regular bath, washing hands with soap before eating and after
using the toilet, brushing teeth, trimming nails, and wearing
clean clothes. Personal hygiene checks the entry of pathogens
of typhoid, amoebiasis, ascariasis, ringworm and many other
infections that travel by the faecal-oral route or by skin
contact.
Public sanitation. Proper disposal of garbage and
excreta, periodic cleaning and disinfection of water reservoirs
and tanks, swimming pools and cisterns, and the use of clean
and covered drains. These measures cut off the route of
water-borne and food-borne diseases such as cholera, typhoid,
amoebiasis and ascariasis.
Safe and clean drinking water. Drinking only boiled,
filtered or chlorinated water; protecting tube-wells and
hand-pumps from contamination; and avoiding open street
beverages prevents water-borne diseases like typhoid, cholera,
amoebiasis and hepatitis A.
Control of vectors and their breeding grounds.
Eradication of mosquito-breeding sources by draining stagnant
water from coolers, tyres, pots and gutters, spraying
insecticides (DDT in older programmes, today pyrethroids),
introducing larvivorous fish such as Gambusia into
ponds, and using mosquito nets and repellents controls
malaria, dengue, chikungunya, filariasis. Similarly, controlling
rats, flies and cockroaches checks plague and many enteric
infections.
Vaccination and immunisation. Routine immunisation
of infants and children against polio, diphtheria, tetanus,
pertussis, measles, mumps, hepatitis-B and tuberculosis
builds active immunity in the population and gives
herd immunity, which protects even the un-immunised.
Health education. Awareness drives through school
programmes, posters, electronic and print media on safe sex,
safe food, hand-washing, oral rehydration, breast-feeding,
and the dangers of self-medication empower people to protect
themselves.
Early diagnosis and treatment. Screening, easy access
to government dispensaries, free essential drugs (DOTS for
tuberculosis, ART for HIV), and the timely isolation of cases
prevent secondary transmission.
Personal hygiene, public sanitation, safe drinking water,
vector control, vaccination, health education and prompt
diagnosis-treatment together form the core public-health shield
against infectious diseases.
AI
Aanya Iyer
M.Sc Microbiology, JNU
Verified Expert
Strategic angle: attack the chain. Every infectious disease
needs a source, a route and a susceptible host.
Public-health measures are easiest to remember if you tie each one
to the link of the chain it breaks.
Attack the source. Isolation of patients (TB ward,
COVID quarantine), prompt treatment of confirmed cases with
the right antibiotics or antivirals, and notification of
infectious diseases to the local health authority dry up the
source of pathogens.
Attack the route. (a) Water-borne: chlorination,
boiling, sand filtration. (b) Air-borne: ventilation, masks
in crowded settings, covering the mouth while sneezing.
(c) Vector-borne: removal of stagnant water, insecticide
spraying, biological control with Gambusia fish, use
of mosquito nets. (d) Food-borne: hygienic kitchens, covered
food, washing fruits and vegetables, pasteurisation.
(e) Sexual: safe sex, screening of donor blood for HIV and
HBV.
Strengthen the host. Universal Immunisation Programme
(UIP) vaccines from birth through adolescence; balanced
nutrition that maintains the body's barriers and immune cells;
breast-feeding of infants for passive antibody transfer; and
treatment of co-morbidities like diabetes that weaken
immunity.
Surveillance and education. Disease registries,
epidemic-alert systems, school awareness on hand-washing and
safe sex, posters in clinics on the danger of self-medication
and indiscriminate antibiotic use.
Why this matters. Most of India's gains in life expectancy
since 1950 come not from new drugs but from these simple
public-health interventions. Smallpox was wiped out by vaccination
alone; polio is on the verge of eradication by the same means.
Break the source, block the route, protect the host: this
three-pronged public-health approach is the safest, cheapest and
most durable safeguard against infectious diseases.
Q 7.2
In which way has the study of biology helped us to control infectious diseases?
Concept used. The control of an infectious disease rests on
three pillars: (i) knowing the pathogen that causes it,
(ii) knowing the life cycle and mode of transmission of
that pathogen, and (iii) designing tools (drugs, vaccines, vector
controls, diagnostic tests) that strike specifically at the
pathogen or its weak link. Each of these pillars rests on biology,
that is, on what microbiology, immunology, biochemistry, molecular
biology and biotechnology have discovered.
Discovery and identification of pathogens.
Microbiology has shown that infectious diseases are caused
by specific organisms: malaria by Plasmodium, typhoid
by Salmonella typhi, cholera by Vibrio cholerae,
TB by Mycobacterium tuberculosis, AIDS by HIV,
amoebiasis by Entamoeba histolytica, ringworm by
Microsporum, Trichophyton, Epidermophyton. Without
this knowledge no targeted control is possible.
Understanding life cycles and transmission.
Parasitology and ecology have mapped the life cycles, like
the Plasmodium cycle between female Anopheles
and humans, and the Ascaris faecal-oral cycle. This
knowledge tells us where to break the cycle (e.g.
kill mosquito larvae, treat drinking water).
Development of drugs and antibiotics. Pharmacology
and biotechnology have given us specific antimicrobials:
chloroquine and artemisinin for malaria, penicillin and
cephalosporins for bacteria, fluconazole for fungal
infections, antiretrovirals (ART) for HIV. Each kills the
pathogen with minimum damage to the host.
Vaccines and immunisation. Immunology has revealed
the antigen-antibody system, allowing scientists to design
vaccines (live attenuated, killed, sub-unit, recombinant DNA
vaccines like Hepatitis B, mRNA vaccines like COVID-19).
Vaccines have eradicated smallpox and have brought polio,
measles and diphtheria under tight control.
Diagnostic technology. Molecular biology has given
rapid, sensitive tests: ELISA for HIV and dengue, Widal for
typhoid, PCR for tuberculosis and COVID-19, microscopy for
malaria. Early diagnosis means early treatment and less
secondary spread.
Vector and reservoir control. Entomology and
ecology have identified vectors and their breeding habits,
leading to integrated vector management: insecticides,
larvivorous fish, biocontrol, and habitat modification.
Genetic engineering and biotechnology. Recombinant
vaccines (Hep B), monoclonal antibodies (for cancer, COVID),
gene therapy and DNA vaccines are direct fruits of modern
biology.
Biology, through microbiology, immunology, pharmacology,
biotechnology and ecology, has given us the pathogens' identity,
their life cycles, the drugs to kill them, the vaccines to prevent
them, the tests to detect them and the controls to interrupt their
transmission. That is how we control infectious diseases today.
AS
Aarav Sharma
Ph.D Molecular Biology, NCBS Bangalore
Verified Expert
Strategic angle: from microscope to molecule. Trace the
arc of biology in three eras and the picture becomes clear.
The microscope era. Leeuwenhoek, Pasteur and Koch
proved that microorganisms cause disease (germ theory). Each
infectious illness was tied to a specific microbe. This
single insight ended centuries of mysticism and made
targeted control even thinkable.
The antibiotic and vaccine era. Fleming's penicillin
(1928) opened the antibiotic era; Jenner's cowpox vaccine
(1796) and the later vaccines for polio, measles, mumps,
rubella and Hep B opened the immunisation era. India's
Universal Immunisation Programme now covers >90% of
children against six killer diseases.
The molecular era. Recombinant DNA technology has
given recombinant Hep B vaccine; monoclonal antibodies treat
cancer and severe COVID-19; PCR delivers diagnoses in hours;
gene therapy is reaching the clinic. Bioinformatics tracks
outbreak strains in near real-time.
Public-health applications. Knowledge of life cycles
(Plasmodium needs water for mosquito breeding; Ascaris
spreads via faecal contamination of soil and water; HIV
needs blood, semen or breast-milk for transmission) lets us
design specific public-health drives: drain stagnant water,
chlorinate the supply, screen blood, distribute condoms.
Why this matters. A century ago, infectious diseases caused
about 40% of all deaths in India. Today they cause less than 15%.
That drop is entirely the work of biology applied to public health.
Biology's progress, from germ theory through antibiotics
and vaccines to recombinant DNA and PCR, has armed humanity with the
specific tools needed to identify, prevent, diagnose and treat every
major infectious disease.
Q 7.3
How does the transmission of each of the following diseases take place?
(a) Amoebiasis (b) Malaria (c) Ascariasis (d) Pneumonia
Concept used.Transmission is the route by which
a pathogen passes from an infected source (a sick person, a carrier
or a contaminated reservoir) to a healthy susceptible host. The
four diseases asked here run on four distinct routes: faecal-oral
(water/food), vector-borne (mosquito bite), faecal-oral (soil/water
contaminated with eggs), and respiratory droplet.
Pathogen + Route, side-by-side
tabularp0.18 p0.30 p0.42
Disease & Pathogen & Transmission route
Amoebiasis & Entamoeba histolytica (protozoan) & Cysts in food/water contaminated by faeces; carried by houseflies.
Malaria & Plasmodium (4 species; P. falciparum most dangerous) & Bite of infected female Anopheles mosquito.
Ascariasis & Ascaris lumbricoides (round-worm) & Ingestion of embryonated eggs from soil/water/vegetables polluted by faeces.
Pneumonia & Streptococcus pneumoniae, Haemophilus influenzae (bacteria) & Inhalation of droplets/aerosols from a sick person; shared utensils.
tabular
(a) Amoebiasis (amoebic dysentery). Caused by the
protozoan Entamoeba histolytica. The pathogen lives
as a cyst in the large intestine of infected people. Cysts
are released in their faeces. When faeces contaminate food
or drinking water, or when houseflies (mechanical vectors)
carry the cysts onto exposed food, a healthy person who
eats or drinks the contaminated material picks up the
infection. Hence faecal-oral transmission through
contaminated food and water; flies act as mechanical
carriers.
(b) Malaria. Caused by Plasmodium species
(P. vivax, P. malariae, P. ovale and the
deadliest P. falciparum). It needs two hosts: a
female Anopheles mosquito and a human. When an
infected female Anopheles bites a healthy human, it
injects sporozoites (the infective form) into the
blood; they enter liver cells, multiply, then infect RBCs.
When a fresh Anopheles bites the patient, it picks up
gametocytes, which fuse and develop in the mosquito
gut. Hence vector transmission through the bite
of an infected female Anopheles mosquito.
(c) Ascariasis. Caused by the intestinal round-worm
Ascaris lumbricoides. Adult worms in the intestine
of an infected person release thousands of eggs that pass
out in the faeces and pollute soil, water, plants and
vegetables. A healthy person who eats raw or poorly washed
vegetables, drinks contaminated water, or puts dirty hands
in the mouth swallows the embryonated eggs and develops the
disease. Hence faecal-oral transmission via soil,
water and vegetables contaminated with eggs.
(d) Pneumonia. Caused chiefly by the bacteria
Streptococcus pneumoniae and Haemophilus
influenzae. The pathogen lodges in the alveoli of the
infected person's lungs and is released in the tiny droplets
that come out when the patient coughs, sneezes or talks. A
healthy person inhales these droplets, or comes into contact
with the patient's utensils, glass or used tissue, and picks
up the bacteria. Hence droplet (air-borne) transmission
through coughing/sneezing and through shared utensils.
Amoebiasis and ascariasis spread by the faecal-oral route
through contaminated food and water; malaria spreads by the bite of
an infected female Anopheles mosquito; pneumonia spreads by
inhaled respiratory droplets from a sick person.
RK
Riya Kapoor
M.Sc Zoology, Banaras Hindu University
Verified Expert
Strategic angle: name pathogen and route together. Pair
each disease with its pathogen first, then state the route. This
structure scores cleanly and never confuses cause with vehicle.
Amoebiasis – pathogen Entamoeba histolytica
(protozoan). Cysts shed in faeces of an infected person
contaminate drinking water and uncooked food (salads, fruits);
houseflies act as mechanical vectors. The healthy person
ingests the cysts and develops amoebic dysentery.
Malaria – pathogen Plasmodium (protozoan).
Transmitted biologically by an infected female Anopheles
mosquito. When the mosquito bites, it injects sporozoites in
saliva. Mosquito control breaks transmission.
Ascariasis – pathogen Ascaris lumbricoides
(round-worm). Embryonated eggs from faeces contaminate soil,
water and vegetables grown in such soil; the healthy person
eats them. Hence faecal-oral. Adequate sanitation and washing
of vegetables stops the cycle.
Pneumonia – pathogens Streptococcus pneumoniae
and Haemophilus influenzae (bacteria). Spread by
droplets when an infected person coughs/sneezes, or through
shared utensils; inhalation by a healthy person seeds the
alveoli. Covering the mouth while coughing and not sharing
utensils breaks transmission.
Why this matters. Two of the four (amoebiasis, ascariasis)
need clean water and sanitation; one (malaria) needs vector control;
one (pneumonia) needs personal respiratory hygiene and vaccination.
The control strategy follows directly from the route.
Faecal-oral for amoebiasis and ascariasis, female
Anopheles bite for malaria, droplet inhalation for pneumonia.
Q 7.4
What measure would you take to prevent water-borne diseases?
Concept used.Water-borne diseases are diseases
whose pathogens travel from sick to healthy people in contaminated
drinking water. Typical examples are typhoid, cholera, amoebiasis,
hepatitis A, polio, ascariasis and several diarrhoeal illnesses.
Prevention works at two ends: (i) stop the pathogen from getting
into the water, and (ii) purify the water before drinking.
Provide clean, treated drinking water. Use municipal
treated water; if unsure, boil drinking water for at least
10minutes to kill bacteria, viruses, protozoan cysts
and worm eggs. Alternatively, treat water with chlorine
tablets, ultraviolet (UV) light, or pass it through a tested
ceramic/RO filter.
Protect water sources from contamination. Keep wells,
tube-wells and hand-pumps covered. Place pit latrines and
soak-pits at least 15m away from any drinking-water
source. Do not allow sewage, animal waste or industrial
effluent to drain into ponds, rivers and reservoirs used for
drinking.
Proper disposal of faeces and sewage. Use proper
toilets connected to septic tanks or a covered drainage
system. Open defecation contaminates soil and rainwater
run-off, which then enters surface water bodies.
Personal hygiene. Wash hands thoroughly with soap
and clean water before preparing or eating food and after
using the toilet. Avoid drinking from open glasses at street
stalls; avoid ice made from untreated water.
Food and kitchen hygiene. Wash fruits and vegetables
with treated water; do not eat cut/peeled fruits sold on the
roadside; cover cooked food to keep flies off; do not store
drinking water in open vessels.
Public sanitation drives. Periodic cleaning and
chlorination of community water tanks; control of houseflies
(which carry pathogens from faeces to food); regular
inspection of water-pipes for leaks (sewage seeps into them
through fractures and creates outbreaks).
Vaccination and prompt treatment. Vaccines for
typhoid, cholera and hepatitis A protect specifically against
water-borne pathogens. Patients of cholera or dysentery
should be treated quickly with oral rehydration solution
(ORS) and appropriate antibiotics to stop further shedding.
Drink only treated/boiled/filtered water; protect drinking
sources from sewage; use covered toilets; wash hands with soap; keep
food and kitchen clean; chlorinate community tanks; and take available
vaccines for typhoid, cholera and hepatitis A.
PB
Pooja Banerjee
M.Sc Biotechnology, AIIMS Delhi
Verified Expert
Strategic angle: kill the cycle at every step from toilet
to glass. A water-borne pathogen travels: infected gut →
faeces → environment (soil, water source) →
piped water/well → glass → healthy gut. Block
any step and you prevent the disease.
Block at the toilet. Provide closed toilets connected
to septic tanks/STP; stop open defecation. Treat the
patient's faeces with bleaching powder before disposal in
outbreak settings.
Block at the source. Locate wells, tube-wells and
rainwater catchments well away from soak-pits and drains.
Maintain a buffer zone around ponds and rivers used for
drinking.
Block at distribution. Repair leaking water pipes,
especially where they cross sewer lines. Maintain residual
chlorine in the piped supply.
Block at point of use. Boil for 10 minutes, or
chlorinate with one halazone tablet per litre, or use a
certified RO/UV filter. Store treated water in a covered
steel pot with a long-handled ladle to avoid hand contact.
Block at the host. Hand-washing with soap, especially
before eating and after the toilet, removes any residual
pathogen at the gateway to the gut. Vaccinate against
typhoid, cholera and hepatitis A in high-risk areas.
Why this matters. Diarrhoeal disease is still a top-three
killer of Indian children. Studies show that supplying chlorinated
piped water plus universal hand-washing alone cut its incidence by
more than half. The measures are cheap, the gains are huge.
Cut the faecal-oral chain at the toilet, at the source, in
distribution, at the point of use and at the host. Boiling/filtering,
clean toilets, hand-washing with soap and selective vaccination
together prevent virtually all water-borne diseases.
Q 7.5
Discuss with your teacher what does `a suitable gene' means, in the context of DNA vaccines.
Concept used. A DNA vaccine (also called a
third-generation vaccine) is a small circular piece of DNA (a
plasmid) carrying the gene that codes for one or more
antigenic proteins of the pathogen we want to vaccinate
against. When the plasmid is injected into a host, the host's own
cells transcribe and translate the gene, the antigen protein appears
on the cell surface, and the host's immune system makes antibodies
and memory cells against it. Hence a suitable gene is the
specific piece of pathogen DNA that, when expressed in the host,
produces a protein that triggers a strong, lasting, protective
immune response without causing disease.
It must code for an antigenic protein of the pathogen.
The gene must encode a protein the immune system recognises
as `non-self', so that B-cells and T-cells respond.
Surface proteins, capsid proteins or envelope glycoproteins
are usual choices (for example the spike-protein gene for
SARS-CoV-2, the HBsAg gene for Hepatitis B virus, the
circumsporozoite-protein gene for Plasmodium).
The protein must elicit protective immunity. Some
antigens make antibodies that bind but do not block the
pathogen; the chosen gene must give a neutralising
response, i.e. the antibodies should actually stop infection
or kill the pathogen.
It must be safe. The gene must not code for any
toxin or any protein that lets the pathogen multiply inside
the host. It is only the antigen, never the whole pathogen.
It must be conserved across strains. The gene's
product should not change easily between strains and seasons,
otherwise the vaccine quickly becomes useless (a problem with
the influenza virus's surface antigens).
It must be efficiently expressed in human cells.
The gene is placed under a strong human-cell promoter
(typically the CMV promoter) so that the host cell makes
plenty of antigen. The gene's sequence is sometimes codon-
optimised for human ribosomes.
It must be small enough to clone into a plasmid.
Practical plasmids carry roughly ≤ 10 kb of insert; a
good vaccine gene is usually 1–3 kb.
A `suitable gene' for a DNA vaccine is a small, conserved,
non-toxic piece of pathogen DNA that codes for an antigenic surface
protein, is efficiently expressed in human cells, and elicits a
strong, lasting and protective (neutralising) immune response.
KM
Karan Mehta
M.Sc Biotechnology, AIIMS Delhi
Verified Expert
Strategic angle: think like a vaccine engineer. You are
shopping for a gene in the pathogen's genome. What do you check?
Antigenicity check. Run the candidate protein
through immunoinformatic prediction or pull data from
infected-patient sera. If their immune system has already
targeted the protein, your vaccine will too. Spike, capsid,
envelope proteins normally pass.
Neutralisation check. Does the antibody to this
protein actually stop infection in cell culture? If not, the
gene is unsuitable, however antigenic. The HIV envelope is
antigenic but most antibodies fail to neutralise; that is
why an HIV DNA vaccine has been hard to make.
Conservation check. Compare the gene across strains
and species. A region conserved across all variants gives a
long-lived vaccine (universal flu vaccines target conserved
stalk regions).
Safety check. The gene must not encode a toxin, an
oncoprotein, an integrase or any virulence factor. It must
not provoke autoimmunity by mimicking a host protein.
Expression check. Add a strong promoter (CMV) and
a polyA tail; codon-optimise; verify protein expression in
a cell line. Without expression, no antigen, no vaccine.
Why this matters. The right gene is the difference between
a life-saving vaccine and a useless plasmid. The criteria above
turn `which gene?' from a guess into a checklist.
The suitable gene is the antigenic, neutralising,
conserved, safe and well-expressed piece of pathogen DNA that, when
made in the host's cells, gives lasting protection without
causing disease.
Q 7.6
Name the primary and secondary lymphoid organs.
Concept used. The lymphoid system is a network of
organs and tissues where the cells of the immune system
(lymphocytes: B and T cells) are produced, mature and act.
Primary lymphoid organs are the sites where immature
lymphocytes are produced and undergo maturation into immuno-
competent B and T cells (i.e. cells able to recognise self from
non-self). Secondary lymphoid organs are the sites where
the matured lymphocytes meet antigens, get activated, multiply
clonally and mount the actual immune response.
[See diagram in the PDF version]
Primary lymphoid organs. (i) Bone marrow
is the main site where all blood cells, including
lymphocytes, are produced. B-lymphocytes mature here in
mammals. (ii) Thymus is a lobed organ near the
heart, beneath the breast-bone. It is large in babies but
shrinks with age (involution). T-lymphocytes are formed in
the bone marrow and then migrate to the thymus, where they
mature. Both bone marrow and thymus also provide the
microenvironment for self-tolerance: lymphocytes that react
against the body's own tissues are eliminated here.
Secondary lymphoid organs. (i) Spleen: a
bean-shaped organ in the upper left abdomen; filters
blood-borne microbes and stores lymphocytes.
(ii) Lymph nodes: bean-shaped, scattered through
the body along lymphatic vessels; trap micro-organisms and
antigens that enter the lymph and tissue fluid.
(iii) Tonsils: at the back of the throat; guard
against pathogens entering through the mouth and nose.
(iv) Peyer's patches of the small intestine.
(v) Appendix. (vi) Mucosa-associated
lymphoid tissue (MALT): located within the lining of the
respiratory, digestive and urogenital tracts; about 50% of
the body's lymphoid tissue lies in the MALT.
Primary lymphoid organs: bone marrow and
thymus. Secondary lymphoid organs: spleen, lymph
nodes, tonsils, Peyer's patches, appendix and MALT.
VR
Vivaan Reddy
M.Sc Biotechnology, AIIMS Delhi
Verified Expert
Strategic angle: factory vs. battlefield. Primary organs
are the factory (make and train soldiers); secondary organs are
the battlefield (where the soldiers meet the enemy antigen).
Factory. Bone marrow makes all lymphocytes and
matures B-cells. Thymus matures T-cells (T = thymus).
Lymphocytes that pass quality control here become
immunocompetent; the rest are killed (negative
selection).
Self-test. If asked `where do B-cells mature?'
→ bone marrow. `Where do T-cells mature?'
→ thymus. `Where do lymphocytes meet antigen?'
→ secondary organs.
Why this matters. Removing the spleen (after trauma) leaves
the patient vulnerable to encapsulated bacteria (pneumococcus,
meningococcus). Thymic dysfunction (DiGeorge syndrome) causes
T-cell deficiency. Each organ's role is a clinical reality.
Bone marrow and thymus are primary; spleen, lymph nodes,
tonsils, Peyer's patches, appendix and MALT are secondary.
Q 7.7
The following are some well-known abbreviations, which have been used in this chapter. Expand each one to its full form:
(a) MALT (b) CMI (c) AIDS (d) NACO (e) HIV
Concept used. The chapter introduces several biomedical
acronyms that recur in immunology and public health. Memorising
both the full form and a one-line meaning is enough for board and
NEET marks.
(a) MALT = Mucosa-Associated Lymphoid Tissue. The
diffuse lymphoid tissue embedded in the mucous lining of the
respiratory, digestive and urogenital tracts. It is a
secondary lymphoid tissue and constitutes about 50%
of the body's total lymphoid tissue.
(b) CMI = Cell-Mediated Immunity. The arm of
acquired immunity executed by activated T-lymphocytes
(rather than circulating antibodies). It is responsible for
defence against intracellular pathogens (viruses,
Mycobacterium) and for the rejection of grafts.
(c) AIDS = Acquired Immuno-Deficiency Syndrome. A
deadly disease caused by HIV, marked by a progressive loss
of helper T-cells, repeated opportunistic infections,
weight loss, swollen lymph glands and ultimately death if
untreated.
(d) NACO = National AIDS Control Organisation. A
body of the Ministry of Health and Family Welfare, Government
of India, set up in 1992 to oversee HIV/AIDS prevention,
diagnosis, treatment (ART) and awareness in India.
(e) HIV = Human Immuno-deficiency Virus. The
retrovirus that causes AIDS. It is an RNA virus with the
enzyme reverse transcriptase; it infects helper T-cells
(CD4+) and macrophages of the human immune
system.
(a) MALT = Mucosa-Associated Lymphoid Tissue;
(b) CMI = Cell-Mediated Immunity;
(c) AIDS = Acquired Immuno-Deficiency Syndrome;
(d) NACO = National AIDS Control Organisation;
(e) HIV = Human Immuno-deficiency Virus.
DJ
Diya Joshi
M.Sc Microbiology, JNU
Verified Expert
Strategic angle: pair acronym with picture. For each
acronym, hold a one-image mental note: MALT → gut lining
patrolled by lymphocytes; CMI → T-cells punching holes in
an infected cell; AIDS → a depleted immune-cell graph;
NACO → red-ribbon awareness drives; HIV →
spiky envelope virus budding from a T-cell. Pictures stick better
than letters.
MALT. Mucosa-Associated Lymphoid Tissue. 50% of
total body lymphoid tissue; first responders at the gut,
airway and urogenital mucosae.
CMI. Cell-Mediated Immunity. Mediated by
T-lymphocytes; targets intracellular pathogens and rejects
foreign tissue grafts.
AIDS. Acquired Immuno-Deficiency Syndrome. Caused
by HIV; defined by CD4+ count <200
cells/μL plus opportunistic infections.
NACO. National AIDS Control Organisation, the apex
body of the Government of India's HIV/AIDS response since
1992.
HIV. Human Immuno-deficiency Virus. Family
Retroviridae, genus Lentivirus; RNA genome reverse-
transcribed and integrated into host DNA.
Why this matters. In NEET and Boards, full-form questions
are easy marks. In the clinic, knowing the acronym is shorthand for
knowing the disease.
MALT, CMI, AIDS, NACO, HIV expanded and defined as above.
Q 7.8
Differentiate the following and give examples of each:
(a) Innate and acquired immunity (b) Active and passive immunity
Concept used.Immunity is the overall ability of
the body to fight disease-causing organisms. It has two broad
divisions based on how the protection is acquired:
innate (present at birth) vs. acquired (developed
during life). The acquired arm further splits into active
(the body itself makes antibodies) vs. passive (ready-made
antibodies are received from outside).
(a) Innate vs. Acquired immunity.
tabularp0.42 p0.50
Innate (non-specific) immunity & Acquired (specific) immunity
Present from birth; inherited from parents. & Develops over the lifetime in response to specific pathogens.
Non-specific: acts on every type of microbe. & Specific: responds to a particular pathogen.
Acts immediately; no time-lag. & Slower (5–14 days for primary response).
No immunological memory; same response every time. & Memory cells remember the pathogen; faster, stronger secondary response on re-exposure.
Four barriers: physical (skin, mucous), physiological (HCl in stomach, lysozyme in tears/saliva), cellular (PMN-leucocytes, monocytes, NK cells, macrophages), cytokine (interferons). & Two arms: humoral (B-cells make antibodies in blood) and cell-mediated (T-cells attack infected cells/grafts). Example: skin keeps microbes out; stomach acid kills swallowed bacteria; lysozyme in tears destroys bacteria in the eye. & Example: antibodies produced after measles infection or after the MMR vaccine; T-cell killing of virus-infected cells; rejection of an unmatched organ graft.
tabular
(b) Active vs. Passive immunity.
tabularp0.42 p0.50
Active immunity & Passive immunity
The host's own immune system makes antibodies on exposure to the antigen. & Ready-made antibodies (antiserum) are received from outside.
Slow to develop (days to weeks) but long-lasting; memory cells form. & Acts at once but is short-lived (a few weeks); no memory.
Examples of natural active immunity: recovery from measles, mumps, chicken-pox. Examples of artificial active immunity: vaccination with polio, MMR, hepatitis-B, COVID-19 vaccine. & Examples of natural passive immunity: IgG antibodies transferred from mother to foetus through the placenta; IgA antibodies in colostrum to a newborn. Examples of artificial passive immunity: anti-tetanus serum (ATS), anti-snake-venom serum, monoclonal antibodies for COVID-19.
tabular
(a) Innate: inborn, non-specific, immediate, no
memory (skin, stomach HCl, lysozyme, phagocytes). Acquired:
develops during life, pathogen-specific, slower, has memory
(antibodies after vaccination/recovery, T-cell graft rejection).
(b) Active: body itself makes antibodies, slow, long-lasting
(vaccination, natural recovery). Passive: ready-made
antibodies given, quick, short-lived (anti-tetanus serum, mother's
milk antibodies).
AK
Ananya Kumar
M.Sc Microbiology, JNU
Verified Expert
Strategic angle: who makes the antibody? If the body itself
makes the antibody, the immunity is active. If the antibody comes
ready-made from outside, the immunity is passive. The same logic,
applied across natural and artificial routes, gives every example.
Innate vs. acquired in one line. Innate is the
bodyguard you are born with; acquired is the bodyguard you
train through experience.
Examples, innate. Skin, mucous, gastric HCl, tear
lysozyme, ciliated airway, phagocytic neutrophils and
macrophages, NK cells, interferons.
Examples, acquired. Antibody response after measles
or mumps, response to a tetanus toxoid booster, T-cell
rejection of an unmatched kidney transplant.
Active immunity (body makes). Natural: recovery from
measles, chicken-pox, mumps. Artificial: every vaccine -
polio, BCG, DPT, MMR, Hep B, COVID-19.
Passive immunity (body receives). Natural: maternal
IgG across the placenta, IgA in colostrum. Artificial:
anti-tetanus serum, anti-rabies serum, anti-snake-venom
serum, monoclonal antibodies (e.g. Casirivimab) for
severe COVID-19.
Why this matters. A new-born is protected for ∼6
months by maternal antibodies (passive). After that, vaccines
(active) take over. Active and passive immunity, working together,
keep a baby alive through the first vulnerable year.
Innate = inborn, non-specific, immediate. Acquired =
learned, specific, slower, memory. Active = body makes the antibody
(vaccine, infection). Passive = body receives the antibody (mother's
milk, anti-tetanus serum).
Q 7.9
Draw a well-labelled diagram of an antibody molecule.
Concept used. An antibody (immunoglobulin, Ig) is
a Y-shaped protein produced by B-lymphocytes in response to a
specific antigen. Each antibody molecule has four polypeptide
chains: two identical light (L) chains and two identical
heavy (H) chains. Because of this H2L2 composition,
the molecule is symbolically written as H2L2. The
two arms of the Y end in identical antigen-binding sites,
which recognise and bind the specific antigen. The chains are held
together by disulphide (-S-S-) bonds. Each
chain has a variable (V) region (the antigen-binding end)
and a constant (C) region (the stem). The five major
immunoglobulin classes are IgA, IgD, IgE, IgG and IgM, distinguished
by their heavy-chain constant regions.
Fig. 7.4, NCERT Class 12 Biology,
Chapter 7 (Human Health and Disease): structure of an antibody
molecule, showing the two heavy chains, two light chains, the
disulphide bonds and the two antigen-binding sites.
Identify the four chains. Two long heavy
chains run as the trunk and inner arm of the Y. Two short
light chains sit on the outside, one alongside each
heavy arm.
Mark the antigen-binding sites. The two upper tips
of the Y, where one light and one heavy chain meet, are the
identical antigen-binding sites. Each binds one antigen
molecule, so a single antibody can bind two antigens.
Mark the disulphide bonds. Several
-S-S- bridges hold the heavy chains
to each other (in the hinge region) and each light chain to
its heavy chain. They keep the four-chain assembly together.
Mark the variable (V) and constant (C) regions.
The V region (the upper part of each arm) is highly variable
across antibodies and gives them their specificity. The C
region (the lower part of the stem) is conserved within each
Ig class and decides effector function. Label the N-terminus
and C-terminus accordingly.
State the formula. Because there are two H and two
L chains, the formula is H2L2.
An antibody is a Y-shaped protein with
H2L2 four-chain composition: 2 heavy + 2 light
chains linked by -S-S- bonds, ending in
two identical antigen-binding sites at the variable (V) tips of
the Y, with the constant (C) stem deciding the immunoglobulin class
(IgA, IgD, IgE, IgG, IgM).
IB
Ishaan Bhat
Ph.D Molecular Biology, NCBS Bangalore
Verified Expert
Strategic angle: dissect by chain, by region, by function.
First name the chains, then the bonds, then the regions, then the
function. The same logic gives a clean labelled drawing every time.
Chains. 2 light (L) chains ≈ 25 kDa each; 2
heavy (H) chains ≈ 50 kDa each. Total mass
≈ 150 kDa. Symbol H2L2.
Bonds. Inter-chain disulphide bonds link L–H and
H–H in the hinge region. Intra-chain disulphide loops give
each chain its globular domain structure.
Regions. VL + VH at the tip = antigen-
binding site (Fab end). CL + CH at the stem = Fc
end, which binds Fc receptors on macrophages and complement
proteins.
Classes. The CH heavy-chain isotype defines the
class: μ in IgM, γ in IgG, α in IgA,
ε in IgE, δ in IgD. Each has a
characteristic effector role (IgG crosses placenta, IgA in
mucosa, IgE in allergy, IgM is the first responder).
Specificity. The V regions form a 3-D pocket
(∼ 10 kDa wide) shaped to fit one antigen epitope. One
clone of B-cell makes only one specificity.
Why this matters. Knowing the parts of an antibody is the
basis of every immunological technique: ELISA, Western blot,
immunofluorescence, antibody therapy for cancer (Rituximab,
Trastuzumab) and for COVID-19 (Casirivimab, Imdevimab).
Y-shaped, four-chain H2L2 protein with
two identical antigen-binding sites at the Fab tips and an Fc
effector stem.
Q 7.10
What are the various routes by which transmission of human immuno-deficiency virus takes place?
Concept used.HIV is a retrovirus that lives
inside cells of the human immune system and inside body fluids
(blood, semen, vaginal secretions, breast-milk). It is fragile
outside the body and cannot spread through air, food, water,
casual contact, mosquitoes, sharing toilets or insect bites. It can
only spread when one of these contaminated body fluids of an
infected person enters the bloodstream of a healthy person. Hence
there are four main routes.
Sexual contact. Unprotected sexual intercourse
(vaginal, anal or oral) with an HIV-infected person is the
commonest route. Semen and vaginal secretions of the infected
partner carry the virus; small abrasions in the mucosa of
the healthy partner let it enter the blood.
Blood and blood products. Transfusion of infected
blood or blood products (plasma, platelets, clotting factors
in haemophiliacs) was a major route before donor screening
became universal. Today, mandatory ELISA screening has
largely closed this route in regulated blood banks.
Sharing of infected needles or syringes. Common
among intravenous drug users who share needles; also a risk
during unsafe medical injections, ear-piercing, tattooing
and acupuncture with poorly sterilised equipment.
Mother-to-child (vertical) transmission. An
HIV-positive mother can transmit the virus to her child:
(i) across the placenta during pregnancy, (ii) through blood
contact during childbirth, or (iii) through breast-milk
during nursing.
HIV does NOT spread by
Mosquito bites, sharing utensils, hugging, shaking hands, swimming
pools, toilet seats, sweat, sneezing, or eating together. Knowing
this is as important as knowing the real routes, because the social
stigma is what kills patients alongside the disease.
HIV spreads through four established routes only:
(i) unprotected sexual contact with an infected partner;
(ii) transfusion of infected blood/blood products;
(iii) sharing of infected needles, syringes or sharp instruments;
(iv) from an infected mother to her child during pregnancy,
delivery or breast-feeding.
TS
Tara Singh
M.Sc Microbiology, JNU
Verified Expert
Strategic angle: fluid carries virus into blood. HIV needs
a contaminated body fluid (blood, semen, vaginal fluid,
breast-milk) of an infected person to physically reach the blood of
a healthy person. The four routes are exactly the four ways such a
contact happens.
Sex. Unprotected vaginal, anal or oral intercourse
with an HIV-positive partner. Use of latex condoms blocks
this route.
Blood. Transfusion of unscreened blood or blood
products; sharing of needles among injecting drug users;
unsafe medical and cosmetic procedures with unsterile
equipment.
Vertical. An infected mother passes the virus to
her baby in utero, during delivery, or through breast-milk.
Antiretroviral therapy of the mother during pregnancy plus
formula feeding (where safe) cuts the risk to below 1%.
Occupational, rare. Needle-stick injuries in
healthcare workers; the risk is small (about 0.3% per
injury) and is reduced further by post-exposure
prophylaxis (PEP).
Why this matters. Each route has a specific block: condom
for sex, screening + needle-exchange for blood, ART + safe delivery
+ formula feeding for mother-to-child. India's NACO programme runs
all three blocks together.
Sexual contact, infected blood/needles and infected
mother to child: the four established HIV transmission routes.
Q 7.11
What is the mechanism by which the AIDS virus causes deficiency of immune system of the infected person?
Concept used. The AIDS virus (HIV) is a
retrovirus: its genome is single-stranded RNA enclosed in
a protein coat surrounded by a lipid envelope studded with
glycoprotein spikes. Inside its capsid it also carries the enzyme
reverse transcriptase. The virus specifically targets
the helper T-lymphocytes (TH cells, also
called CD4+ T-cells) and macrophages of the human
immune system. Repeated cycles of infection, replication and
killing of TH cells progressively destroy this central
co-ordinator of the immune response, leaving the patient unable to
defend against secondary infections. That progressive loss is the
immunodeficiency of AIDS.
[See diagram in the PDF version]
Entry. After transmission, HIV enters macrophages.
Its envelope glycoprotein (gp120) binds specifically to the
CD4 receptor on macrophages and helper T-cells,
and the virus is taken into the cell.
Reverse transcription. Inside the cell, the viral
enzyme reverse transcriptase copies the single-
stranded RNA genome into a double-stranded DNA. This step
gives the retrovirus its name (the reverse of the usual
DNA -> RNA flow).
Integration. The newly synthesised viral DNA enters
the nucleus of the host cell and integrates into the host
chromosome (catalysed by viral integrase). The virus now
lives as a permanent passenger of the cell.
Replication and budding. The infected cell is
directed by the integrated viral DNA to produce new viral
RNA genomes and viral proteins. These assemble at the cell
membrane and bud off as new virions, which infect
more macrophages and helper T-cells.
Destruction of helper T-cells. Each round of
replication destroys the infected TH cell.
Because TH cells are the central
co-ordinators of the immune response (they activate B-cells
for antibody production and activate cytotoxic T-cells), a
progressive fall in their number cripples both humoral and
cell-mediated immunity. Normal CD4+ count is
∼ 1000 cells/μL; in AIDS it drops below 200.
Opportunistic infections. With the immune defence
gone, organisms that the body normally easily controls
(Mycobacterium tuberculosis, Pneumocystis
jirovecii, Cryptococcus, Toxoplasma,
cytomegalovirus, Candida) cause severe and recurrent
infections, and certain cancers (Kaposi's sarcoma) develop.
These are the clinical symptoms of AIDS.
HIV binds the CD4 receptor of helper
T-cells/macrophages, reverse-transcribes its RNA into DNA, integrates
into the host chromosome, replicates and buds out, killing the
TH cell. The progressive loss of TH
cells cripples the coordination of both humoral and cell-mediated
immunity, leaving the patient open to opportunistic infections and
cancers - the immunodeficiency we call AIDS.
KN
Krishna Nair
Ph.D Molecular Biology, NCBS Bangalore
Verified Expert
Strategic angle: a retrovirus that hijacks the conductor.
The helper T-cell is the conductor of the immune orchestra; HIV is
a parasite that lives in the conductor and slowly silences him,
after which the orchestra goes to pieces.
Receptor. HIV's gp120 envelope spike fits the
CD4 receptor on helper T-cells and macrophages
(and the coreceptor CCR5/CXCR4). This is the specificity
that makes the virus immune-tropic.
Genome flow. A retrovirus flips the central dogma:
RNA ->[reverse transcriptase] DNA inside the host.
That DNA integrates into the host genome as a
provirus, becoming a permanent part of the cell.
Slow burn. For months to years the provirus lies
relatively quiet (the asymptomatic phase). Stress signals
and cytokines turn on transcription, and the cell starts
making viral particles, which kill it.
Numbers. The body initially replaces lost
TH cells, but the bone marrow cannot keep pace
with the rate of destruction. Over 5–10 years the
CD4+ count crashes from ∼ 1000 to
< 200/μL. Below 200, AIDS is declared.
Consequence. Without TH cells, the
immune orchestra cannot mount an effective response. Common
microbes become deadly: Pneumocystis pneumonia, TB,
cryptococcal meningitis, candidiasis, CMV retinitis,
Kaposi's sarcoma.
Why this matters. Knowing the mechanism gave us
antiretroviral therapy: reverse-transcriptase inhibitors
(zidovudine, tenofovir), protease inhibitors and integrase
inhibitors. Triple-drug ART now turns AIDS from a death-sentence
into a chronic illness with near-normal life expectancy.
HIV binds CD4+ T-cells, reverse-transcribes
its RNA to DNA, integrates as provirus, replicates, and kills the
TH cell. Progressive loss of TH cells
cripples both arms of immunity → opportunistic
infections → AIDS.
Q 7.12
How is a cancerous cell different from a normal cell?
Concept used. A normal cell grows and divides
under the strict control of two systems: contact inhibition
(cells stop dividing once they touch their neighbours) and
cell-cycle checkpoints (the cell only divides when
growth signals and DNA repair allow it). A cancerous cell
(neoplastic cell) is one in which these controls have broken down:
it divides repeatedly, ignores neighbour signals, refuses to die
when damaged, and may break free of its original site.
Loss of contact inhibition. Normal cells stop
dividing on touching neighbours, so a culture of normal
cells forms a single layer (monolayer). Cancer cells ignore
this contact signal and pile up on each other, forming
multilayered, disorganised masses.
Uncontrolled, rapid division. Normal cells divide
a limited number of times and only when needed (replacement,
repair). Cancer cells divide continuously and rapidly,
producing a mass of cells called a tumour.
Loss of differentiation. Normal cells differentiate
into specialised cell types (e.g. liver cells, skin cells).
Cancer cells lose their normal shape, size and function;
they look immature (anaplastic) under the microscope.
Failure to die (apoptosis). Normal cells with
damaged DNA trigger programmed death (apoptosis). Cancer
cells escape apoptosis because regulatory genes such as
p53 are mutated; damaged cells survive and accumulate.
Invasion and metastasis (in malignant tumours).
Normal cells stay in their organ of origin. Malignant
cancer cells break out of the primary site, invade
surrounding tissues, enter blood and lymph, and seed
distant organs - this is metastasis. Benign tumours, by
contrast, stay encapsulated.
Angiogenesis. Malignant tumours secrete factors
(VEGF) that recruit new blood vessels to feed themselves.
Genetic changes. Cancer cells carry mutations in
proto-oncogenes (converted to oncogenes that drive
growth) and in tumour-suppressor genes (e.g.
p53, RB, which normally restrain growth). Normal cells
have intact copies.
Other features. Cancer cells often have abnormal
chromosome numbers (aneuploidy), high telomerase activity
(so they do not senesce), altered metabolism (Warburg
effect), and elevated tumour markers (CEA, PSA, AFP).
tabularp0.42 p0.50
Normal cell & Cancerous cell
Shows contact inhibition; divides only when needed. & No contact inhibition; divides continuously.
Limited number of divisions; senesces. & Almost unlimited divisions; immortal.
Specialised (differentiated). & Poorly differentiated (anaplastic).
Stays in its tissue of origin. & Can invade and metastasise.
Undergoes apoptosis if damaged. & Escapes apoptosis (p53 inactive).
Normal chromosome number. & Aneuploidy, chromosomal rearrangements.
Normal blood supply. & Stimulates new blood vessels (angiogenesis).
Genome intact. & Mutated proto-oncogenes and tumour-suppressor genes.
tabular
Cancer cells differ from normal cells in losing contact
inhibition, dividing uncontrollably, losing differentiation,
escaping apoptosis, sustaining their own blood supply, harbouring
mutated oncogenes and tumour-suppressor genes, and (in malignant
tumours) invading neighbouring tissues and metastasising to distant
organs.
YV
Yash Verma
M.Sc Biotechnology, AIIMS Delhi
Verified Expert
Strategic angle: rules-followed vs. rules-broken. A normal
cell follows the rules of the tissue community: divide only when
asked, stop when neighbours say so, die if damaged, stay home. A
cancer cell breaks all of them.
Rule 1: Divide only when asked. Normal cells need
growth signals (growth factors). Cancer cells synthesise
their own or have constitutively active receptors (Ras
mutations).
Rule 2: Stop when neighbours say so. Normal cells
feel contact inhibition; cancer cells ignore it.
Rule 3: Die if damaged. Normal cells with damaged
DNA undergo p53-mediated apoptosis. Cancer cells have
p53 mutations and survive.
Rule 4: Stay home. Normal epithelial cells stay
within the basement membrane. Cancer cells secrete proteases
(MMP9), break out and seed distant organs (metastasis).
Rule 5: Run out of divisions. Normal cells exhaust
their telomeres after ∼ 50 divisions. Cancer cells
reactivate telomerase and become immortal.
Why this matters. Every modern cancer drug, from imatinib
to nivolumab, targets a specific broken rule. Diagnosis (biopsy +
histopathology + molecular markers) and therapy follow directly
from these differences.
Cancer cells lose contact inhibition, divide without
limit, lose differentiation, escape apoptosis, build their own
blood supply and (in malignancy) invade and metastasise to distant
organs. Normal cells obey all these rules; cancer cells break them
all.
Q 7.13
Explain what is meant by metastasis.
Concept used.Metastasis is the most dangerous
property of malignant tumours. It is the process by which cancer
cells of a primary (original) tumour break away, travel through the
bloodstream and/or lymphatic system to distant parts
of the body, settle there and grow into new (secondary) tumours.
The word literally means a change of place. It is the
single most important reason why cancer is hard to treat - once
metastatic spread has happened, surgery alone cannot remove all the
disease.
[See diagram in the PDF version]
Detachment. Cancer cells in a malignant primary
tumour lose cell-to-cell adhesion (down-regulated
E-cadherin) and break out of their tissue of origin.
Invasion. They secrete proteolytic enzymes
(matrix metalloproteinases) that digest the basement
membrane and surrounding extracellular matrix, allowing
the cells to push into nearby tissues.
Intravasation. The cells enter the lumen of blood
capillaries or lymphatic vessels.
Circulation. Tumour cells travel as
circulating tumour cells (CTCs) through blood or lymph.
Most are destroyed by the immune system; a few survive.
Extravasation. A surviving cell adheres to the
endothelium of a distant capillary, squeezes between
endothelial cells, and enters the new tissue.
Colonisation. The cell multiplies at the new site,
recruits new blood vessels (angiogenesis), and grows into
a secondary (metastatic) tumour. Common sites of
metastasis are the liver, lungs, bones and brain.
Metastasis is the spread of cancer cells from a malignant
primary tumour, through the blood or lymphatic system, to distant
organs, where they form new (secondary) tumours. It is the property
that makes malignant cancer especially dangerous, because the
disease is no longer confined to one site.
SD
Sneha Desai
M.Sc Microbiology, JNU
Verified Expert
Strategic angle: travel itinerary of a cancer cell. Think
of a malignant cell as an unwanted traveller. It packs (loses
adhesion), exits the building (basement membrane), boards transport
(blood/lymph), gets off at a far station (extravasation) and rents
a new flat (colonisation).
Pack. Loss of E-cadherin lets cells separate.
Exit. MMP-secretion dissolves the basement
membrane.
Transport. Entry into capillaries or lymph
vessels.
Survive the trip. Resist immune attack and
haemodynamic shear stress.
Disembark. Adhere to vessel wall at a distant
organ, transmigrate through the endothelium.
Settle. Colonise the new tissue; trigger
angiogenesis to feed the new colony; grow into a secondary
tumour.
Why this matters. 90% of cancer deaths are from metastasis,
not from the primary tumour. Treatments that block any of the six
steps (e.g. anti-angiogenics, MMP inhibitors, checkpoint inhibitors)
are an active area of research.
Metastasis is the journey of malignant cells from the
primary tumour, through blood/lymph, to distant organs, where they
form secondary tumours - the property that defines malignancy.
Q 7.14
List the harmful effects caused by alcohol/drug abuse.
Concept used.Drug/alcohol abuse is the use of
drugs (opioids, cannabinoids, cocaine, hallucinogens, tobacco) and
alcohol for purposes other than medical, in amounts and
frequencies that harm the user, the family and society. The harm
acts at three levels: (i) the body of the user, (ii) the user's
mind and behaviour, (iii) the user's family and society.
Immediate physical effects. Reckless behaviour,
impaired judgement, accidents on the road, vandalism,
violence. Heroin and alcohol overdose can cause respiratory
depression and death. Loss of inhibition leads to unsafe
sex, raising the risk of HIV and hepatitis B/C.
Long-term effects on the body.
Liver: chronic alcohol use causes fatty liver,
alcoholic hepatitis and cirrhosis; long-term opioid use
damages the liver too.
Heart and lungs: tobacco causes hypertension,
atherosclerosis, coronary artery disease, chronic
bronchitis, emphysema and lung cancer.
Nervous system: chronic abuse causes memory
loss, dementia, peripheral neuropathy and Wernicke–
Korsakoff syndrome (in alcoholics).
Reproductive system: reduced fertility, impotence
in males, foetal alcohol syndrome in babies of alcoholic
mothers (low birth weight, mental retardation, facial
anomalies).
Infectious diseases: HIV, hepatitis B and C
spread through shared needles among intravenous drug
users.
Psychological effects. Dependence and addiction,
depression, anxiety, paranoia, hallucinations (with
cannabinoids), suicidal tendency, and a sharp drop in
academic and work performance.
Withdrawal effects. Once dependent, stopping the
drug suddenly produces severe nausea, sweating, tremors,
muscle pain, hallucinations and seizures; this withdrawal
can be life-threatening.
Tolerance and escalation. The body adapts so that
the same dose stops giving the same `kick'; the user takes
progressively larger doses, increasing the risk of
overdose and toxicity.
Family and social effects. Disturbed family
relationships, financial ruin, child neglect, domestic
violence, school drop-out, and loss of employment.
Generations of `addicts of addicts' if the cycle is not
broken.
Crime and societal cost. To finance the habit, an
addict may steal or sell stolen goods, sell illegal drugs,
engage in prostitution. Drug trafficking and gang violence
weaken the social fabric.
Use of performance-enhancing drugs in sport.
Anabolic steroids cause acne, mood swings, depression,
liver damage, kidney failure, masculinisation in females
(facial hair, deepened voice, menstrual irregularities),
feminisation in males (breast enlargement, shrunken
testes), aggression and premature heart disease.
Drug and alcohol abuse harm the body (liver cirrhosis,
heart disease, lung damage, brain damage, HIV/hepatitis from shared
needles), the mind (addiction, depression, hallucinations, suicide),
the family (financial ruin, neglect, violence) and society (crime,
loss of productivity). They also raise the risk of overdose, foetal
damage and premature death.
AC
Aditya Chatterjee
M.Sc Biotechnology, AIIMS Delhi
Verified Expert
Strategic angle: four concentric circles. Imagine four
circles widening around the user - self, family, peers, society.
Each gets damaged by drug abuse in characteristic ways.
Family. Disturbed relationships, child neglect,
domestic violence, financial bankruptcy, loss of trust.
Foetal alcohol syndrome in unborn children of addicted
mothers.
Peers. Spread of the habit; pressure to share
needles; involvement in trafficking; school drop-outs.
Society. Crime to finance the habit (theft,
prostitution); reduced productivity; healthcare burden;
organised drug trafficking and gang violence.
Why this matters. The total social cost of substance abuse
is enormous (lost lives, lost work, healthcare bills). Prevention
through early education, family support and timely de-addiction is
cheaper and far more effective than treatment of long-standing
addiction.
Drug/alcohol abuse damages the user's body (liver, heart,
lungs, brain, reproductive system), the user's mind (addiction,
depression, suicide), the family (neglect, violence, foetal damage)
and society (crime, productivity loss, healthcare burden).
Q 7.15
Do you think that friends can influence one to take alcohol/drugs? If yes, how may one protect himself/herself from such an influence?
Concept used. Adolescence is a stage where the urge to
belong is strong and the brain's risk-reward circuitry is still
maturing. Peer pressure, the influence of friends and
classmates, is one of the leading reasons that teenagers
first try a drug or a drink. Studies and the NCERT text
itself note that the company we keep is the single most
important external factor in adolescent drug initiation. Hence the
honest answer is yes, friends can strongly influence one to take
alcohol or drugs, especially during early teenage.
How peer pressure operates. An adolescent wants to
fit in, be accepted, be seen as `cool' or grown-up. When
the peer group experiments with cigarettes, alcohol or
drugs, the urge not to be left out, the fear of being
teased, and the temptation of `just trying once' often win
over good sense.
Curiosity and adventure-seeking. Teenagers seek
novelty, take risks and like to challenge rules. Friends
amplify this curiosity: `try it once and see, nothing will
happen'.
Imitation of role-models. Older siblings, popular
seniors and celebrities glamorised in films or social media
are imitated. A friend who looks up to such a figure passes
the influence on.
Recognise the moment of choice
Almost every addiction begins with one moment when a friend says,
``Try this''. Knowing in advance that this moment will come and
deciding the answer in advance is half the protection.
How to protect oneself.
Choose friends with care. Friendships built around
sports, reading, music, dance, debate or community service
give the same sense of belonging without the drug. Avoid
groups where substance use is a routine `fun'.
Be assertive without being aggressive. A firm,
polite `No, thanks' practised in advance is usually enough.
One does not have to argue or apologise. True friends will
accept the refusal.
Build self-esteem and self-identity. A teenager
with strong self-respect, a sport or hobby and clear goals
does not need a drug to feel adult. Parents, teachers and
counsellors can help by acknowledging the student's
achievements and giving responsibility.
Channel curiosity and energy into healthy
outlets. Sports, music, art, NCC, NSS, scouts, debate,
trekking, environmental clubs. These give a real `high'
of achievement and friendship.
Talk to parents and teachers without fear. Open
communication with adults at home and at school is a
strong safety net. If something has already been tried,
admitting it early is much safer than hiding it.
Seek help early. Counsellors, NACO helpline,
de-addiction centres, family physicians. The earlier one
seeks help, the easier the way back.
Learn the facts about drugs. Knowing what
cigarettes, alcohol, cannabis and opioids actually do to
the body and mind (the harmful effects listed in Q14)
replaces glamour with realism.
Yes, friends - especially during adolescence - are a
strong influence on drug or alcohol initiation. The way to protect
oneself is to choose friends with care, learn to say a firm `No',
build self-esteem and goals, channel energy into sports/hobbies,
talk openly with parents and teachers, learn the facts about
drugs, and seek counselling early if needed.
MP
Meera Pillai
M.Sc Microbiology, JNU
Verified Expert
Strategic angle: yes, but plan the defence. Accept the
risk plainly and then list the seven defences. This direct structure
is what examiners want.
Acceptance. Yes, peer pressure is a leading cause
of teenage substance use, recognised by WHO, NCERT and
every public-health agency.
Choice of company. Spend time with friends who
share constructive interests.
Refusal skills. `No' is a complete sentence.
Practise it with parents/siblings.
Self-worth. Build identity through achievement,
sport, art, leadership. Self-respect is the strongest
immune system against peer pressure.
Healthy outlet. Channel curiosity, energy and
adventure into sport, music, trekking, debating, theatre.
Open communication. Talk to parents and teachers
without fear of judgement.
Information. Read about what drugs actually do
(Q14 effects).
Professional help. Counsellors, NACO helpline,
de-addiction centres are available and confidential.
Why this matters. Schools and parents who teach refusal
skills, build self-esteem and keep dialogue open cut substance-use
rates among their teens by more than half. Prevention is teachable.
Yes, peers influence first use. Defence: good company,
firm `No', strong self-esteem, healthy hobbies, open talk with
parents/teachers, factual knowledge of drug harms, early
professional help.
Q 7.16
Why is that once a person starts taking alcohol or drugs, it is difficult to get rid of this habit? Discuss it with your teacher.
Concept used. Alcohol and drugs of abuse act on the
reward pathway of the brain (the meso-limbic dopaminergic
pathway, including the nucleus accumbens and the ventral tegmental
area). They flood it with the neurotransmitter dopamine, far
above the levels released by natural rewards like food, music or
friendship. With repeated use the brain adapts to this artificial
surge, producing two stubborn phenomena: tolerance
(progressively larger doses are needed to feel the same kick) and
dependence (the body and mind need the drug to
feel normal). Together they make stopping extremely hard.
Tolerance. On repeated exposure, dopamine receptors
in the reward pathway down-regulate (their number falls).
The same dose now produces a smaller effect, so the user
takes a larger dose to feel the previous `kick'. This
escalation traps the user in an ever-rising spiral of use.
Physical dependence. The body alters its own
biochemistry to function in the constant presence of the
drug. When the drug is stopped, the altered biochemistry
produces withdrawal symptoms- tremors, sweating,
cramping, nausea, vomiting, seizures, severe anxiety,
sometimes hallucinations and even death. The simplest way
to make these symptoms go away is to take the drug again.
Psychological dependence (craving). The brain
learns to associate the drug with relief from stress,
boredom or sadness. The memory of pleasure becomes so
strong that even years after the body has detoxed, a
familiar place, friend or smell can trigger an intense
craving and bring the user back to use (relapse).
Reward pathway rewiring. Natural rewards (food,
music, friendship) stop feeling rewarding because the brain
has reset its baseline to the drug. The user feels flat
and joyless without the substance, deepening the
dependence.
Social factors. Continued company with using
friends, easy availability of the drug, family discord,
unemployment, and stigma around seeking help all keep
pulling the person back to the substance.
Triggers and relapse. Even after de-addiction,
triggers such as stress, a known location, an old friend,
or simply the time of day at which the user once consumed
the drug can fire the craving. This is why relapse is
common and why long-term support (counselling, family,
de-addiction groups) is essential.
Because alcohol and drugs hijack the brain's reward
pathway, the user develops tolerance (progressively larger doses
needed for the same effect), physical dependence (severe withdrawal
on stopping), psychological dependence (deep cravings) and a
rewired reward circuit. These changes, combined with social
pressures and easy availability, make it extremely hard to break
the habit once it has been formed.
RG
Rohit Gupta
Ph.D Molecular Biology, NCBS Bangalore
Verified Expert
Strategic angle: three locks on the door. Tolerance,
dependence and craving are three locks the drug puts on the way out.
Each must be opened to stop using.
Lock 2: Physical dependence. Withdrawal is so
unpleasant that users restart the drug just to feel
normal. Breaking it needs supportive medical care:
rehydration, sedatives for seizures, gradual taper,
substitution (methadone, buprenorphine) where indicated.
Lock 3: Psychological dependence. Cues from the
past trigger cravings. Breaking it needs cognitive-
behavioural therapy, group support (AA, NA), and a
rebuilt social environment far from old triggers.
Add social glue. Family support, employment,
purpose. Recovery rates double when the recovering person
has a job, a home and an accepting community.
Prevent relapse. Identify triggers, plan
responses, stay close to a support group long after the
last use. Recovery is a lifelong project, not a one-time
event.
Why this matters. `Just stop' is poor medical advice.
Recognising addiction as a brain disease with three locks helps
both the patient and the family approach recovery scientifically.
Drug abuse rewires the reward pathway, producing
tolerance, physical and psychological dependence. The combined
neurobiology and social environment make stopping very hard, and
recovery needs medical, psychological and social support
together.
Q 7.17
In your view what motivates youngsters to take to alcohol or drugs and how can this be avoided?
Concept used. A youngster's first contact with alcohol or
drugs is rarely random. It is driven by a cluster of push
factors (curiosity, peer pressure, family stress, social
glamourisation) and pull factors (an immediate thrill of
relaxation or excitement). Avoidance therefore needs an equally
multi-pronged response.
What motivates youngsters.
Curiosity and thrill-seeking. Adolescents are
biologically wired to seek novelty and adventure. `What if
I try it once?' is a powerful pull.
Peer pressure. Friends who already use drugs may
tease, dare or persuade. Wanting to fit in beats common
sense (also covered in Q15).
Family stress. Frequent quarrels, lack of warmth
at home, unrealistic academic expectations, divorce or
neglect push the child to look for escape.
Failure to cope with academic and personal
pressures. Heavy syllabus, competition, exam fear and
peer comparison drive some adolescents to relaxants
(alcohol, cannabinoids) or stimulants (cocaine,
amphetamines).
Glamourisation in media. Films, web series, music
videos and social media often depict drinking and drug use
as `cool', adult or rebellious. Young viewers imitate
their on-screen idols.
Easy availability. If alcohol, cigarettes and
gateway drugs (cannabis) are easily available near schools
and colleges, experimentation is far more likely.
Misinformation. `Everyone does it', `It is
harmless', `I can stop whenever I want'. Such myths,
spread by older peers and the internet, lower the barrier
to first use.
Need for an identity and rebellion. Adolescence
is a phase of identity formation. Some youngsters use
drugs as a way to assert independence from parents and
teachers.
How this can be avoided.
Early education about drugs. School syllabi
should include factual information on what each drug does
to the body and brain, replacing glamour with realism
(the Q14 effects).
Strong, warm and communicative families. Parents
who listen, who set reasonable expectations, who share
meals and conversations with their children, who watch
for early signs (changing friends, mood swings, falling
grades, money missing) and who address them gently -
these families have the lowest rates of drug abuse.
Teachers and counsellors as a safety net. Trained
school counsellors, accessible without fear of punishment,
can catch trouble early. Anonymous helplines (NACO,
de-addiction centres) extend the net.
Avoid peer-pressure traps. Teach refusal skills,
encourage choice of constructive peer groups, build
self-esteem (see Q15).
Channel energy positively. Sports, music, dance,
debate, NCC, NSS, scouts, art, social work. Real
achievement is a far stronger natural high than any
drug.
Address root stress. Mental-health counselling
for anxiety, depression, exam fear or family discord
treats the cause before the youngster reaches for a drug.
Regulate availability. Strict enforcement of laws
on the sale of alcohol and tobacco to minors; control of
narcotics; quick action on drug peddlers near schools
and colleges.
Looking for danger signs. A sudden drop in
grades, withdrawal from family, isolated lifestyle,
unkempt appearance, weight loss, mood swings, missing
money, changed peer group - any of these calls for a
gentle adult conversation, not punishment.
Professional help on time. Once experimentation
has begun, professional de-addiction (medical detox +
counselling + family + group support) gives the best
chance of recovery. The earlier the intervention, the
better.
Role of media. Responsible portrayal in films and
social media; warning labels; campaigns by celebrities;
public-service messaging (NACO posters, NSS drives).
Curiosity, peer pressure, family stress, academic
pressure, media glamourisation, easy availability and the need for
an identity together motivate youngsters to try alcohol or drugs.
Avoidance needs early factual education, warm families, accessible
school counsellors, refusal skills, channelling of energy into
sports and arts, mental-health support, strict regulation of
availability, early detection of warning signs, prompt professional
help and responsible media.
AR
Aditi Rao
M.Sc Biotechnology, AIIMS Delhi
Verified Expert
Strategic angle: matched pairs. For every push factor that
takes a youngster towards drugs, there is a counter-force that
takes them away. Pair them up and the answer becomes both balanced
and memorable.
Curiosity→ replace with adventure
sports, science clubs, real experiments.
Peer pressure→ choose company well;
practise saying `No' politely.
Family stress→ family counselling;
warm, regular dialogue at home.
Academic pressure→ realistic
expectations; coaching on time-management; mental-health
counselling.
Media glamour→ media literacy in
school; warning labels; responsible storytelling by film
industry.
Easy availability→ strict enforcement
of age-laws on alcohol/tobacco; tighter narcotics control.
Need for identity→ leadership roles
in school clubs, social work, sport teams.
Misinformation→ factual NCERT-level
education on what drugs really do.
Early signs→ trained school
counsellors, accessible helplines, non-judgemental
teachers.
Professional help→ NACO, government
de-addiction centres, AA/NA groups.
Why this matters. A youngster surrounded by good company,
warm parents, alert teachers, channels for energy, and accessible
counsellors is at very low risk of substance abuse. Society can
build all of these.
Curiosity, peers, family stress, academic pressure,
media glamour, easy availability and identity-formation drive
youngsters to substance use. Education, families, schools, sport,
counselling, regulation and responsible media together prevent
it.
NCERT Solutions for Class 12 Biology: All Chapters
Browse the chapter-wise Class 12 Biology NCERT Solutions across the full 2026-27 syllabus on Collegedunia.
Human Health and Disease Class 12 Biology NCERT Solutions FAQs
Ques. Where can I download Class 12 Biology Chapter 7 Human Health and Disease NCERT Solutions PDF?
Ans. You can download the Human Health and Disease Class 12 Biology NCERT Solutions PDF directly from this page. Both the Normal and HD versions are free and aligned with the 2026-27 NCERT.
Ques. Are these NCERT Solutions aligned with the 2026-27 syllabus?
Ans. Yes. This page reflects the current 2026-27 syllabus for Class 12 Biology. NCERT did not trim Human Health and Disease, so all 17 exercise questions are still examinable for CBSE Boards and NEET.
Ques. How many questions are there in the Human Health and Disease NCERT exercise?
Ans. The end-of-chapter exercise has 17 numbered questions plus 10 acronym expansions inside Q7. The PDF carries step-by-step worked answers to every one of them.
Ques. What is the NEET weightage of Class 12th Biology Chapter 7 Human Health and Disease?
Ans. NEET pulls 3 to 5 questions from this chapter every year. Immunity (helper T-cells, antibody isotypes) and cancer types are the two highest-yield sub-topics.
Ques. Which is the most-asked NCERT question from Human Health and Disease in CBSE Boards?
Ans. Q8 (draw a labelled antibody diagram) and Q10 (mechanism by which AIDS virus causes immune deficiency) are the two most frequently repeated. Both have appeared in at least three of the last five CBSE Board papers.
Ques. How do the NCERT Solutions help with NEET preparation for this chapter?
Ans. Every solution flags the exact phrase NEET asks verbatim: helper T-lymphocyte, sporozoite, metastasis, oncogene, so the same answer doubles as a one-mark MCQ recall sheet. The Q7 acronym list and the antibody isotype mnemonic ("GAMED") map directly to NEET assertion-reason items.
Ques. Are diagrams included in the Class 12 Biology Chapter 7 NCERT Solutions PDF?
Ans. Yes. The antibody Y-structure (Q8), Plasmodium life cycle (Q3), and HIV replication cycle (Q11) come fully labelled with examiner-grade markings ready to copy into the board answer script.
Ques. What is the difference between active and passive immunity in NCERT Class 12 Biology?
Ans. Active immunity is when the body produces its own antibodies after antigen exposure (vaccination, infection): slow but long-lasting. Passive immunity is when ready-made antibodies are injected (tetanus antitoxin, mother's milk colostrum): fast but short-lived. The PDF answer to Q8(c) shows the full comparison table.











































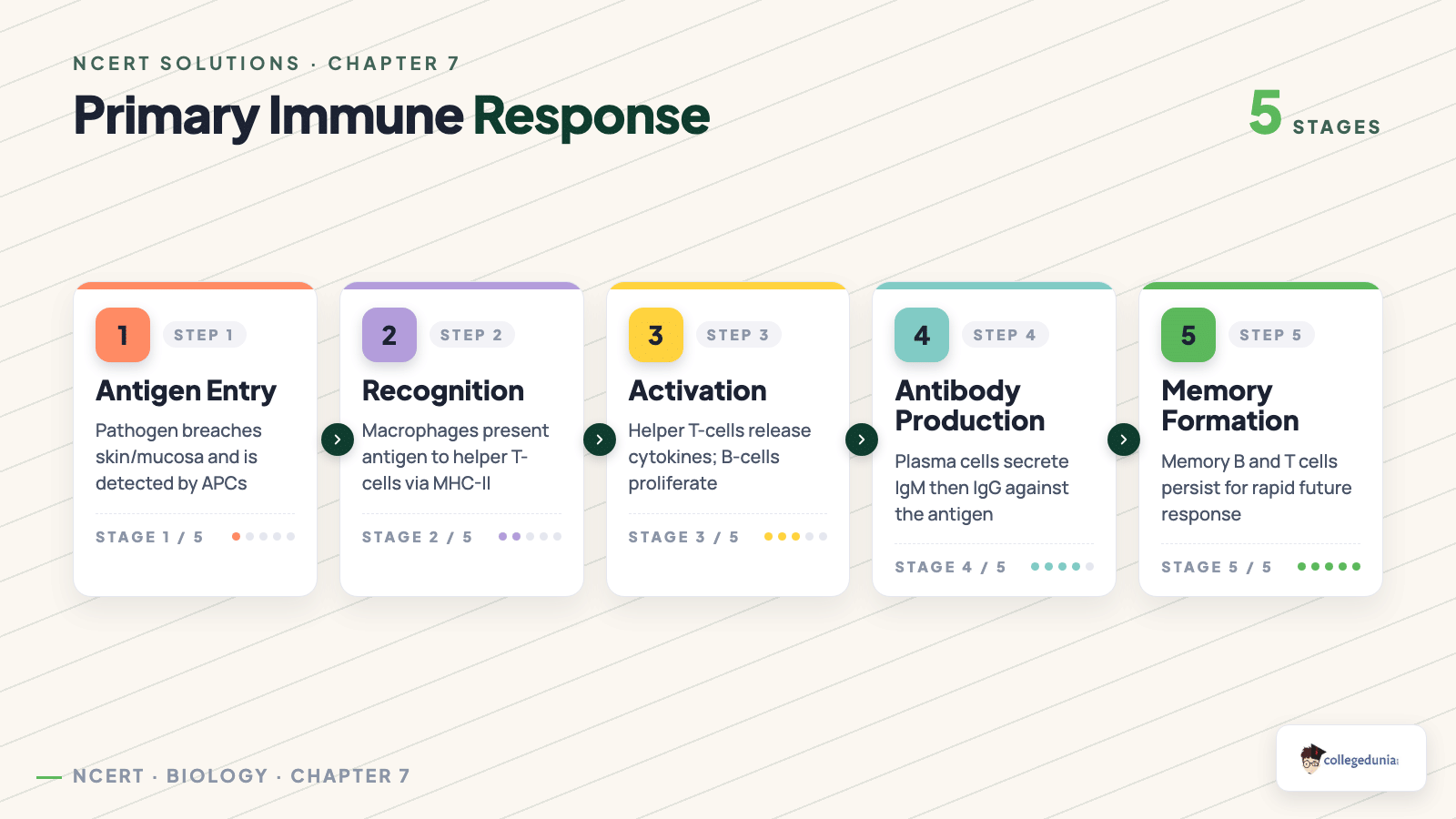
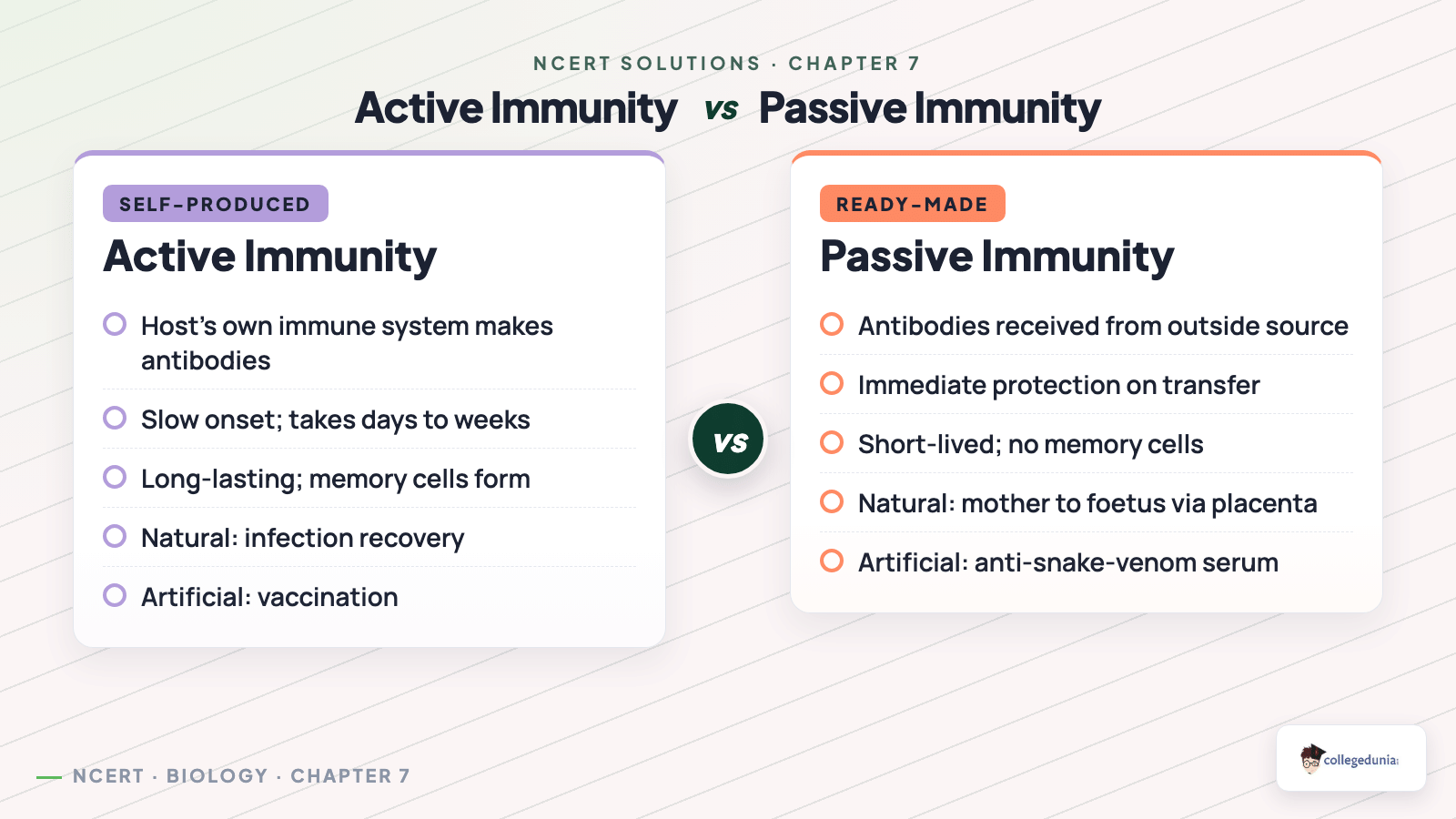
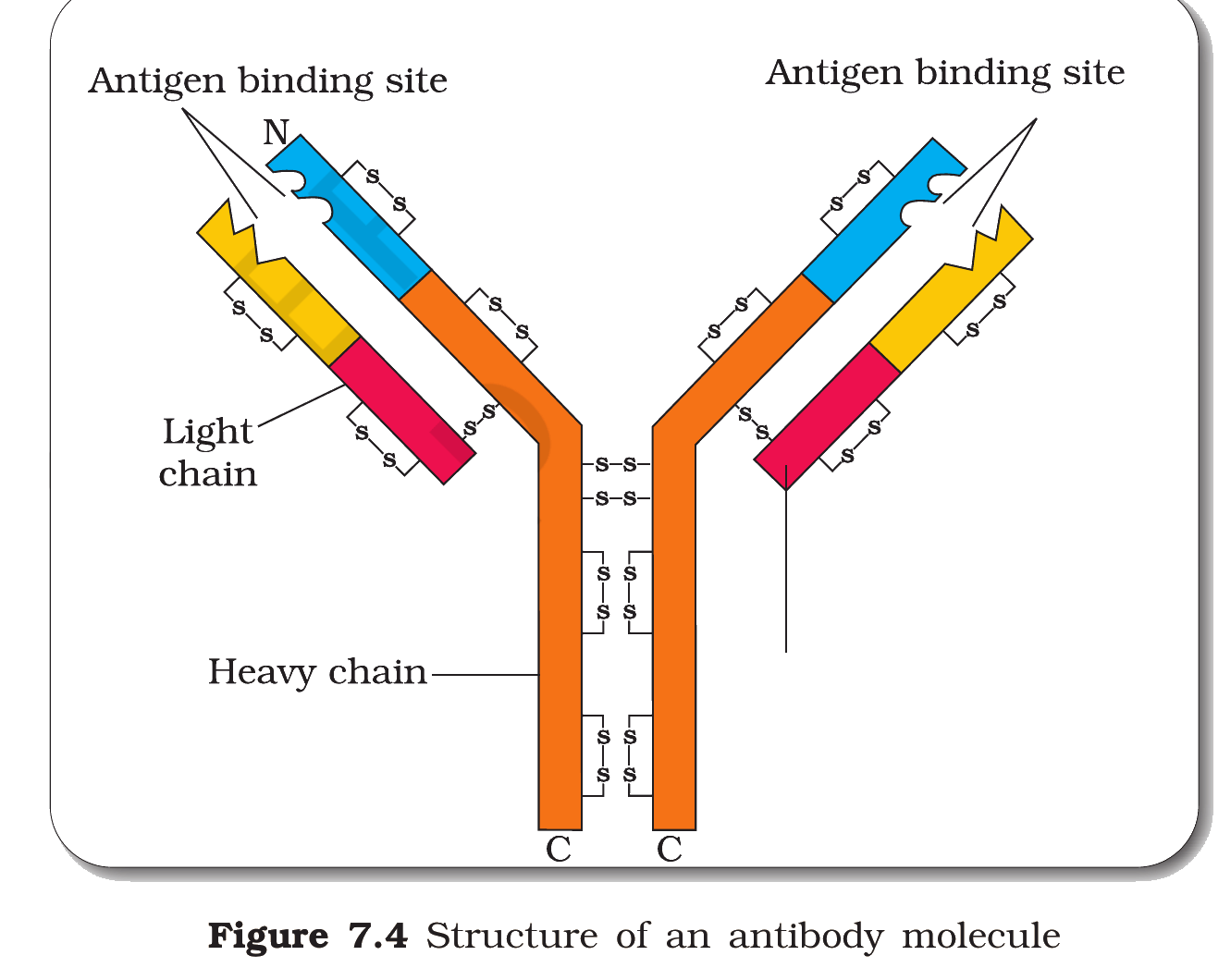


Comments