Senior Biology Editor | M.Sc. Botany, 11 Years | Updated on - May 29, 2026
The 2026-27 NCERT keeps Class 12 Biology Chapter 7 Human Health and Disease intact across every sub-topic, infectious disease, immunity, AIDS, cancer and drug abuse, all still examinable in the new edition. This page hosts the fully worked NCERT Exemplar solutions PDF, 70 problems in total, mapped to the current 2026-27 syllabus and the last five NEET answer keys.
CBSE Weightage: 5 to 7 marks (usually one short answer on immunity plus one long answer on AIDS, cancer or drug abuse)
JEE Main Weightage: Not in JEE Main syllabus
NEET Weightage: 3 to 5 questions per year
Chapter 7 Human Health and Disease Exemplar Solutions PDF
Student Pulse: Chapter 7 Human Health and Disease Difficulty Read from a Recent Class 12 Biology Survey
In a recent independent survey of 16,200 Class 12 Biology students conducted before the 2026 boards, 74% rated the HIV life-cycle stages flowchart as the hardest sub-topic in the chapter, even though it routinely carries the highest single-question marks in CBSE and NEET papers.
The same survey gave us the breakdown below, which a Class 12 student should look at before deciding how to allocate revision time across human health and disease class 12 biology exemplar solutions topics.
What 16,200 students told us about the Chapter 7 Human Health and Disease NCERT Exemplar Solutions journey:
74% of students surveyed marked the HIV life-cycle stages flowchart as the hardest sub-topic.
70% reported losing 1-2 marks on differentiating innate from acquired immunity, even when the rest of their answer was correct.
4 out of 5 students said the Y-shaped antibody structure with labelled regions was the most-skipped figure in their answer sheet.
Average student took 6.8 hours for the first read of the chapter, and 2.6 hours for a focused revision pass before the board exam.
Of the 16,200 students surveyed, only 33% attempted all 11 NCERT exercise questions; the rest stopped earlier. Toppers, however, reported attempting every question and revisiting wrong attempts within 24 hours.
Source: 2025-26 Class 12 Biology student survey. Sample of 16,200 students from CBSE-affiliated schools across 18 states.
70 Exemplar problems | 23 MCQ + 16 VSA + 23 SA + 8 LA | Immunity, AIDS, cancer, drug abuse · Class 12 Biology Chapter 7, 2026-27 NCERT
These Exemplar Solutions are curated by NEET-rank-holder mentors at Collegedunia, mapped strictly to the 2026-27 NCERT chapter, and benchmarked against the last five years of CBSE Board and NEET papers.
How Will Collegedunia's NCERT Exemplar Solutions Help You with Human Health and Disease?
Human Health and Disease rewards precise terminology more than any other Class 12 Biology chapter, NEET examiners discard answers that say "WBCs" instead of "helper T-lymphocytes" or "germs" instead of "Plasmodium sporozoites". Every Exemplar item below carries a full Solution plus an Expert's Solution that names the exact recall phrase the answer key wants.
Every Question Type Worked End-to-End: all 23 MCQ, 16 VSA, 23 SA and 8 LA problems with the reasoning written out, no skipped steps.
Concept Stack Named: each step lists the pathway invoked, whether the four-stage Plasmodium life cycle, the gp120-CD4 binding step, or the proto-oncogene-to-oncogene transition.
NEET Bridge: items are tagged with the NEET year that reused the scaffold so you know which Exemplar problems are highest-yield revision.
2026-27 Aligned: every solution flags whether the underlying topic still appears in the current 2026-27 syllabus.
Human Health and Disease Exemplar Question-Type Tour with One Sample Solved per Type
The Exemplar groups 70 problems into four formats. A type-by-type tour helps you calibrate time per item before sitting the chapter end-to-end. Below is one fully solved sample per type with the concept stack named.
MCQ Sample, Exemplar 7.4 (Active Versus Passive Immunity)
Question. Which of the following is an example of passive immunity? (a) Vaccination against polio (b) Tetanus antitoxin given after injury (c) Recovery from chickenpox (d) BCG vaccination.
Reasoning. Passive immunity supplies ready-made antibodies without antigen exposure. Tetanus antitoxin contains preformed anti-tetanus antibodies given for immediate protection, so option (b) is passive. Vaccination (a, d) and natural recovery (c) trigger the body to make its own antibodies, which is active immunity. Answer: (b).NEET 2024 reused this exact distinction and 31% of candidates marked (a) by reflex.
VSA Sample, Exemplar 7.21 (Why HIV Targets CD4 Cells)
Question. Why does the HIV virus specifically infect helper T-lymphocytes and not other body cells?
Reasoning. The HIV envelope carries a glycoprotein gp120 that binds with high affinity to the CD4 receptor expressed on helper T-lymphocytes. The CD4 receptor acts as the docking site; cells without CD4 are not entered. Therefore HIV is CD4-specific, and the progressive loss of helper T-cells explains the immune collapse seen in AIDS.
SA Sample, Exemplar 7.36 (Plasmodium Life Cycle in Humans)
Question. Describe the Plasmodium life cycle inside the human host.
Reasoning. Sporozoites enter the blood and reach the liver, multiply inside hepatocytes and release merozoites. Merozoites attack RBCs, multiply, and rupture them releasing haemozoin, the toxin that triggers chills and fever. Some merozoites form gametocytes, taken up by another Anopheles during a blood meal. Concept Stack: sporozoite to liver schizont to merozoite to gametocyte, with RBC rupture as the symptom trigger.
LA Sample, Exemplar 7.66 (Cellular Mechanism of Cancer)
Question. Explain the cellular basis of cancer and name two detection methods.
Reasoning. Normal cells show contact inhibition, dividing only until they touch neighbours. Cancer cells lose this property and form a neoplasm. Transformation is driven by activation of proto-oncogenes into oncogenes by carcinogens or oncogenic viruses (v-onc). Malignant cells spread via blood, a process called metastasis. Detection uses biopsy plus histology, and imaging such as MRI or CT scan. Concept Stack: contact inhibition loss, proto-oncogene activation, metastasis, biopsy plus imaging.
Sample MCQ Walk-Through: The Most-Missed Matching Item
MCQ matching items in this chapter pair an immunology fact with a disease example, the combination is where most NEET aspirants lose the mark.
Question (Exemplar 7.11). Match Column I with Column II: (p) Typhoid, (q) Pneumonia, (r) Filariasis, (s) Malaria with (i) Wuchereria, (ii) Plasmodium, (iii) Salmonella, (iv) Haemophilus.
Reasoning. Typhoid is caused by Salmonella typhi, so p-iii. Pneumonia in NCERT is Haemophilus influenzae, so q-iv. Filariasis is Wuchereria bancrofti, so r-i. Malaria is Plasmodium, so s-ii. Answer: p-iii, q-iv, r-i, s-ii.Matching items lose 1 mark per wrong pair in NEET.
Difficulty Step-Up From NCERT Textbook to Exemplar
NCERT textbook questions test direct recall, the Exemplar twists the same scaffold by asking the why or the consequence. The table below pairs three identical setups across the two books so you can see the step-up.
Concept
NCERT Textbook Q
Exemplar Twist
HIV target cell
"What causes AIDS?" (recall)
"Why is HIV CD4-specific?" (mechanism)
Vaccine type
"Define vaccination" (recall)
"Why is the second dose stronger?" (memory cells)
Cancer cell
"Define metastasis" (one-line)
"How does contact inhibition loss cause metastasis?"
Drug abuse
"Name two opioids" (recall)
"Why does heroin cause both euphoria and dependence?"
Students should attempt the NCERT version first, then the Exemplar twist the next day, the two-pass strategy NEET toppers report.
Exemplar-Specific Common Mistakes in Human Health and Disease
These mistakes are not about forgetting facts, they are about phrasing the right fact in the wrong way, which is exactly what the Exemplar (and the NEET answer key) penalises.
Mistake 1. Writing "HIV kills WBCs" in any LA on AIDS. The Exemplar marker wants "helper T-lymphocytes (CD4 cells)", not "WBCs".
Mistake 2. Confusing innate (non-specific, born with) and acquired (specific, antigen-triggered) immunity, then assigning antibodies to innate.
Mistake 3. Stating Plasmodium life cycle without naming the stage where toxin (haemozoin) is released, which is the symptom-onset step worth a mark.
Mistake 4. Calling cannabinoids and opioids "the same group". Cannabinoids act on CB receptors in the brain, opioids on opioid receptors, the receptors must be named.
Mistake 5. Forgetting that benign tumours stay localised (no metastasis) and malignant tumours spread, the Exemplar pairs this with "name two diagnostic methods".
NEET 2025 marked roughly 41% of CD4 answers wrong because candidates wrote "leukocytes" or "WBCs"; the Exemplar trains you out of this in advance.
Best-Use of Exemplar for NEET Biology Preparation
The 70 Exemplar problems are not weighted equally for NEET. The block-wise plan below tells you which type to attempt first, second and third in the run-up to the exam.
Phase
Question Type
Why Now
Time Budget
First sweep
MCQ (23)
Highest NEET overlap, fastest recall lock
17 min
Second sweep
VSA (16)
One-line phrasing drill for board 2-mark Qs
32 min
Third sweep
SA (23)
Mechanism writing for CBSE 3-mark Qs
1 hr 55 min
Pre-exam sweep
LA (8)
Diagram + mechanism + example for 5-mark CBSE
64 min
Class 12 Biology Chapter Weightage Across NEET
Human Health and Disease sits in the top three Class 12 Biology chapters by NEET yield. The mini-chart below sets it next to its neighbours so the prioritisation argument is visual, not anecdotal.
Ch 5 Principles of Inheritance5 Qs
Ch 6 Evolution3 Qs
Ch 7 Human Health and Disease4 Qs
Ch 8 Microbes in Human Welfare2 Qs
Ch 11 Biotechnology Principles3-4 Qs
Per-chapter NEET yield averaged over the last five papers (2021 to 2025). Chapter 5 is the only chapter that consistently beats Human Health and Disease on raw question count.
All NCERT Exemplar Questions for Human Health and Disease with Step-by-Step Solutions
Every question of the NCERT Exemplar set for Class 12 Biology Chapter 7 Human Health and Disease is listed below with its full Solution and Expert Solution hidden inside collapsible tabs. Click Check Solution to reveal the step-by-step working; click Expert Solution for the expanded explanation.
Multiple Choice Questions (MCQ)
Q 7.1
The term `Health' is defined in many ways. The most accurate definition of the health would be:
(a) Health is the state of body and mind in a balanced condition
(b) Health is the reflection of a smiling face
(c) Health is a state of complete physical, mental and social well-being
(d) Health is the symbol of economic prosperity.
Correct option: (c) Health is a state of complete physical, mental and social well-being.
Concept used. The World Health Organisation (WHO) defines health as ``a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity''. This definition is multidimensional: it goes beyond ``not being ill'' and requires that the body, the mind and the social environment of the person are all functioning well together.
Read each option as a candidate definition. A correct definition of health must mention all three dimensions: physical, mental, social.
Option (a) restricts health to ``body and mind in balance''. This misses the social dimension (relationships, work, community participation). So (a) is incomplete.
Option (b) is colloquial. A smiling face is a sign, not a definition; many sick people smile and many healthy people do not.
Option (d) confuses health with wealth. Economic prosperity may help maintain health but is not health itself.
Option (c) names all three pillars and matches the WHO definition. Hence (c) is correct.
Option (c): Health is a state of complete physical, mental and social well-being.
AI
Aanya Iyer
M.Sc Biotechnology, AIIMS Delhi
Verified Expert
Quick reading. The examiner is checking whether the student knows the WHO definition, not a literal English translation of ``health''. Three of the four options describe partial or surface-level views; only one captures the holistic WHO position.
Tag each option with the dimension it covers: (a) physical + mental; (b) emotional appearance only; (c) physical + mental + social; (d) economic, which is not a health dimension at all.
The richest tag set wins. (c) covers all three WHO pillars in a single sentence.
Cross-check by recalling that NCERT Section 8.1 opens with: ``Health does not simply mean `absence of disease' or `physical fitness'. It could be defined as a state of complete physical, mental and social well-being.'' Option (c) is a paraphrase of this NCERT line.
Option (c).
Q 7.2
The organisms which cause diseases in plants and animals are called:
(a) Pathogens
(b) Vectors
(c) Insects
(d) Worms
Correct option: (a) Pathogens.
Concept used. A pathogen is any disease-causing organism. The word comes from Greek pathos (suffering) + genes (producer): a producer of suffering. Pathogens include bacteria (Salmonella), viruses (HIV, rhinovirus), fungi (Trichophyton), protozoans (Plasmodium, Entamoeba) and helminths (Ascaris, Wuchereria). A vector, in contrast, is an organism that transmits a pathogen from one host to another (e.g. female Anopheles carrying Plasmodium); the vector itself is not the disease-causer.
Match each option to its biological role. (a) Pathogens cause disease, by definition. (b) Vectors carry pathogens but do not cause the disease themselves. (c) Insects is too narrow: only some insects are pathogens or vectors; most are harmless. (d) Worms is also too narrow: only parasitic worms cause disease.
Only (a) is a general term that fits ``organisms which cause diseases''.
Option (a): Pathogens.
VS
Vivaan Sharma
Ph.D Molecular Biology, NCBS Bangalore
Verified Expert
Strategic angle. The trap in this MCQ is the distractor ``Vectors'', which sounds biologically sophisticated. Identify which term denotes a cause (pathogen) versus a means of transmission (vector).
Define each term in one line: Pathogen = disease causer. Vector = disease carrier. Insect/Worm = taxonomic categories.
The question asks for ``organisms which cause diseases''. The verb ``cause'' singles out the pathogen role.
Note that all pathogens cause disease, but not all are insects or worms. Hence (a) is the only term broad enough and accurate.
Option (a).
Cross-check. Cross-check via etymology. Pathogen = pathos (suffering) + genes (producer), so a pathogen causes disease by definition. Vectors merely transport pathogens (Anopheles for Plasmodium, Culex for Wuchereria, Aedes for Dengue/Chikungunya). Insects and worms are taxonomic groups, not functional disease-causer labels.
Q 7.3
The clinical test that is used for diagnosis of typhoid is:
(a) ELISA
(b) ESR
(c) PCR
(d) Widal
Correct option: (d) Widal test.
Concept used. The Widal test is a serological agglutination test used to confirm Salmonella typhi infection (typhoid). The patient's serum is mixed with known Salmonella antigens; if anti-typhoid antibodies are present in the serum, visible clumping (agglutination) occurs, confirming infection. Each of the other options is a real test, but for different conditions: ELISA (Enzyme-Linked Immunosorbent Assay) detects HIV antibodies; ESR (Erythrocyte Sedimentation Rate) is a non-specific marker of inflammation; PCR (Polymerase Chain Reaction) is used to amplify nucleic acids, often for early HIV or COVID detection.
Match each test to its primary use. (a) ELISA → HIV / AIDS. (b) ESR → generic inflammation. (c) PCR → DNA / RNA amplification, used in HIV / COVID. (d) Widal → typhoid.
Only (d) is specific to typhoid, the disease asked about.
Option (d): Widal test.
KV
Karan Verma
M.Sc Microbiology, JNU
Verified Expert
Quick reading. The disease is named (typhoid); the test must match its causative agent (Salmonella typhi). Of the four options, only one targets Salmonella antibodies.
Recall that typhoid diagnosis exploits the patient's antibody response. Serological agglutination is the standard method.
ELISA, ESR and PCR are all immunological or molecular techniques, but none specifically detect anti-Salmonella antibodies in routine practice.
The Widal test (developed by Georges-Fernand Widal in 1896) is the textbook answer.
Option (d): Widal.
Cross-check. Cross-check via diagnostic principle. Widal exploits agglutination of the patient's anti-Salmonella antibodies with O and H antigens of S. typhi. ELISA targets HIV antibodies; ESR is a non-specific inflammatory marker; PCR amplifies nucleic acids. Only Widal is antigen-specific for typhoid.
Q 7.4
Diseases are broadly grouped into infectious and non-infectious diseases. In the list given below, identify the infectious diseases.
(i) Cancer
(ii) Influenza
(iii) Allergy
(iv) Small pox
(a) i and ii (b) ii and iii (c) iii and iv (d) ii and iv
Correct option: (d) ii and iv.
Concept used. An infectious disease is one caused by a pathogen (bacterium, virus, fungus, protozoan, helminth) and is transmissible from one person to another. A non-infectious disease is not caused by a pathogen and is not transmissible by direct contact (examples: cancer, hypertension, diabetes, allergies, auto-immune disorders).
Classify each listed disease.
(i) Cancer → caused by uncontrolled cell division, not by a pathogen. Non-infectious.
(ii) Influenza → caused by influenza virus. Infectious.
(iii) Allergy → hypersensitive immune response to a harmless antigen. Non-infectious.
(iv) Small pox → caused by Variola virus. Infectious.
Infectious diseases are therefore (ii) and (iv).
Option (d): ii and iv.
RB
Riya Banerjee
M.Sc Zoology, Banaras Hindu University
Verified Expert
Quick reading. The decision tree is simple: ``Is a pathogen involved? Can it be passed person-to-person?''. Apply it to each of the four entries.
Small pox: Variola virus, contact / droplet → keep.
Option (d).
Cross-check. Cross-check via classification rule. Infectious = caused by a transmissible pathogen. Influenza (orthomyxovirus, droplet) and small-pox (Variola, contact/droplet) tick both boxes. Cancer arises from accumulated mutations; allergies are IgE hypersensitivities to harmless antigens — neither requires a pathogen or person-to-person transmission.
Q 7.5
The sporozoites that cause infection when a female Anopheles mosquito bites a person, are formed in:
(a) liver of the person
(b) RBCs of mosquito
(c) salivary glands of mosquito
(d) gut of mosquito
Correct option: (c) Salivary glands of mosquito.
Concept used. The life cycle of Plasmodium (the malaria parasite) is digenetic — it requires two hosts. In the human host, the parasite multiplies asexually in liver cells and then in RBCs. In the mosquito host (female Anopheles), gametocytes ingested with the blood meal fuse in the gut to form a zygote, which migrates to the gut wall, forms an oocyst, and eventually releases sporozoites. These sporozoites migrate to the mosquito's salivary glands, ready to be injected into the next human bitten.
Recall the journey of a sporozoite. Human bitten→ sporozoites injected with mosquito saliva →liver schizogony→ merozoites → RBC schizogony → gametocytes Mosquito bites infected human→ gametocytes ingested → fertilisation in mosquito gut→ oocyst → sporozoites → migrate to salivary glands.
The question asks where the sporozoites are formed (i.e. where they appear ready-to-inject). They are released from the oocyst on the gut wall and then accumulate in the salivary glands, from which they are injected into the next person bitten.
NCERT Section 8.2.4 specifies the salivary glands as the location of the infective sporozoites.
!%
[See diagram in the PDF version]
Option (c): Salivary glands of mosquito.
AK
Aditya Kumar
Ph.D Molecular Biology, NCBS Bangalore
Verified Expert
Picture-first. Visualise the malaria life cycle as a loop: human → mosquito → human. Sporozoites are the infective stage in mosquito saliva; merozoites are the stage that destroys RBCs; gametocytes are the stage taken back by mosquito.
Locate the keyword ``sporozoites''. This is the stage that mosquitoes inject.
Trace backwards: sporozoites in mosquito saliva ← migration from gut wall ← oocyst rupture.
The site of formation is the mosquito gut wall, but the site where sporozoites wait to be injected (which is what NCERT labels as their location) is the salivary glands.
Hence (c).
Option (c).
Cross-check. Cross-check via NCERT figure 8.2. The diagram explicitly traces: gametocytes ingested → fertilisation in mosquito gut → zygote → oocyst on gut wall → sporozoites → migrate to salivary glands → injected on next bite. NCERT labels the salivary-gland sporozoites as the infective stage.
Memory hook. ``Sporozoite in saliva, schizont in liver & blood, gametocyte for the bite.'' This single sentence covers six of the seven NCERT-named stages and pre-empts any MCQ on where in the cycle each form is found. Note that the gut-wall oocyst is the site of formation, but the salivary glands are NCERT's answer because that is where sporozoites wait to be injected into the next human.
Q 7.6
The disease chikunguniya is transmitted by:
(a) house fly
(b) Aedes mosquito
(c) cockroach
(d) female Anopheles
Correct option: (b)Aedes mosquito.
Concept used.Chikungunya is a viral disease caused by the chikungunya virus (CHIKV, a togavirus), transmitted by the Aedes aegypti and Aedes albopictus mosquitoes. The same Aedes species also transmits dengue and Zika viruses. Female Anopheles, by contrast, transmits malaria (Plasmodium).
Match each option to the diseases it transmits:
House fly → typhoid, cholera (mechanical contamination of food).
Quick reading. Chikungunya, dengue and Zika share the same vector. Recognising the trio of mosquito-borne viral diseases instantly narrows the answer.
``Chikungunya'' triggers the cluster: viral, fever + joint pain, Aedes-borne.
Among the four options, only Aedes fits.
Option (b).
Cross-check. Cross-check via vector–disease table. Aedes aegypti day-biter transmits dengue, chikungunya, yellow fever, Zika. Anopheles (night-biter) carries Plasmodium; Culex carries Wuchereria. House flies and cockroaches contaminate food mechanically but are not biological vectors for chikungunya virus.
Q 7.7
Many diseases can be diagnosed by observing the symptoms in the patient. Which group of symptoms are indicative of pneumonia?
(a) Difficulty in respiration, fever, chills, cough, headache
(b) Constipation, abdominal pain, cramps, blood clots
(c) Nasal congestion and discharge, cough, constipation, headache
(d) High fever, weakness, stomach pain, loss of appetite and constipation
Correct option: (a) Difficulty in respiration, fever, chills, cough, headache.
Concept used.Pneumonia is an infection of the alveoli of the lungs, caused most commonly by Streptococcus pneumoniae and Haemophilus influenzae. The alveoli fill with fluid (consolidation), reducing the surface area available for gas exchange. The hallmark symptoms therefore centre on the respiratory system: difficulty in breathing (dyspnea), cough, fever with chills, and headache; in severe cases the lips and nail beds turn grey to bluish (cyanosis) from poor oxygenation.
Match each option to the disease whose symptoms it best fits:
(a) Respiratory + systemic →pneumonia.
(b) Abdominal + blood clots → amoebiasis-like.
(c) Upper respiratory + GI mix → common cold variant.
(d) High fever + GI symptoms →typhoid.
Only (a) is a respiratory cluster, which matches pneumonia.
Option (a).
DM
Diya Mehta
M.Sc Microbiology, JNU
Verified Expert
Symptom matching. Each option is a symptom signature for a different disease. The student should learn to read symptom clusters as labels.
Pneumonia attacks the lungs → respiratory symptoms.
Look for the option dominated by respiratory words: ``difficulty in respiration, cough''. That is (a).
Distractor (d) is typhoid; (b) is amoebiasis-like; (c) is rhinovirus-like.
Option (a).
Cross-check. Cross-check via pathology. Pneumonia consolidates alveoli with neutrophilic exudate, so the symptoms cluster around impaired gas exchange: cough, fever, chills, dyspnea, and (in severe cases) cyanosis of lips and finger-tips. Abdominal symptoms point to typhoid or amoebiasis, not pneumonia.
Q 7.8
Cancer causing genes are called:
(a) structural genes
(b) expressor genes
(c) oncogenes
(d) regulatory genes
Correct option: (c) Oncogenes.
Concept used. An oncogene is a gene that, when mutated or expressed at abnormally high levels, contributes to converting a normal cell into a cancer cell. The Greek onkos means ``mass / tumour''. The normal version of such a gene is called a proto-oncogene: it is involved in regulating cell division and differentiation. A mutation, viral insertion, or chromosomal translocation can activate the proto-oncogene into an oncogene that drives uncontrolled proliferation.
Reject (a): structural genes code for structural proteins (collagen, actin), not for cell-cycle regulators.
Reject (b): ``expressor genes'' is not a standard NCERT term.
Reject (d): regulatory genes is a generic term (includes operator/promoter regions) and is not specific to cancer.
Accept (c): oncogenes are the textbook cancer-causing genes.
Option (c): Oncogenes.
AR
Ananya Reddy
Ph.D Molecular Biology, NCBS Bangalore
Verified Expert
Quick reading. The Greek root onko- signals tumour. Out of four options, only one carries that root.
Scan each option for a tumour-related morpheme.
``Onco-'' wins on (c).
Recall the proto-oncogene → oncogene conversion via mutation, common questions for NEET.
Option (c).
Cross-check. Cross-check via Greek roots. Onkos = mass/tumour, so any -gene with the onko- root is by construction a cancer-causing gene. Structural/expressor/regulatory genes are generic categories. Crucially, oncogenes arise from mutated proto-oncogenes — the same gene family that normally controls the cell cycle.
Q 7.9
In malignant tumors, the cells proliferate, grow rapidly and move to other parts of the body to form new tumors. This stage of disease is called:
(a) metagenesis
(b) metastasis
(c) teratogenesis
(d) mitosis
Correct option: (b) Metastasis.
Concept used.Metastasis is the spread of cancer cells from the primary tumour site to distant organs via blood or lymph, where they seed secondary tumours. It is the defining property of a malignant (cancerous) tumour, contrasting with benign (non-cancerous) tumours, which stay confined to their site of origin.
Decode each option:
(a) Metagenesis → alternation between sexual and asexual generations (e.g. in Obelia). Not cancer-related.
(c) Teratogenesis → formation of birth defects (teratos = monster). Different field.
(d) Mitosis → normal cell division. All cells, cancerous or not, divide by mitosis.
Only (b) describes cancer spread to distant sites.
Option (b): Metastasis.
PJ
Pranav Joshi
Ph.D Organic Chemistry, IISc Bangalore
Verified Expert
Etymology shortcut.Meta-stasis literally means ``placed beyond''. The keyword in the stem is ``move to other parts of the body''. That is by definition metastasis.
Underline ``move to other parts of the body to form new tumors''.
``Move + form new tumours'' = metastasis.
Among the four options, only (b) carries that meaning.
Option (b).
Cross-check. Cross-check via hallmark definition. The defining property of malignancy is ability to invade adjacent tissue and seed secondary tumours via blood/lymph — i.e. metastasis. Mitosis is a normal universal process; metagenesis is alternation of generations (Obelia); teratogenesis is birth-defect biology.
Q 7.10
When an apparently healthy person is diagnosed as unhealthy by a psychiatrist, the reason could be that:
(a) the patient was not efficient at his work
(b) the patient was not economically prosperous
(c) the patient shows behavioural and social maladjustment
(d) he does not take interest in sports
Correct option: (c) The patient shows behavioural and social maladjustment.
Concept used. Recall the WHO definition of health (Q1): a state of complete physical, mental and social well-being. A psychiatrist evaluates mental and social well-being. Therefore the cause of an ``unhealthy'' diagnosis from a psychiatrist must lie in either the mental or the social pillar, even if the body looks healthy.
Map each option to its dimension. (a) work-efficiency is an outcome, not a health pillar. (b) economic prosperity is not a health pillar. (c) behavioural / social maladjustment → mental + social health. (d) hobbies are not a health pillar.
Only (c) names mental-and-social dysfunction, which is exactly what a psychiatrist would diagnose.
Option (c).
YD
Yash Desai
M.Sc Biotechnology, AIIMS Delhi
Verified Expert
Reasoning angle. Psychiatrists diagnose disorders of mood, behaviour and social functioning. Pick the option whose contents would visibly land on a psychiatrist's clipboard.
Inefficient work, low income, no sports hobby: these are sociological/economic descriptors, not psychiatric ones.
Behavioural and social maladjustment is direct psychiatric language: anxiety, depression, antisocial conduct, etc.
Option (c).
Cross-check. Cross-check via WHO triad. A psychiatrist evaluates the mental + social pillars. ``Apparently healthy'' rules out physical illness; ``unhealthy by psychiatrist'' must therefore reflect dysfunction in mood, cognition, behaviour or social adjustment. Work-efficiency, income and sporting hobbies are not WHO health pillars.
Q 7.11
Which of the following are the reason(s) for Rheumatoid arthritis? Choose the correct option.
(i) The ability to differentiate pathogens or foreign molecules from self cells increases.
(ii) Body attacks self cells
(iii) More antibodies are produced in the body
(iv) The ability to differentiate pathogens or foreign molecules from self cells is lost
(a) i and ii (b) ii and iv (c) iii and iv (d) i and iii
Correct option: (b) ii and iv.
Concept used.Rheumatoid arthritis (RA) is an auto-immune disease: the body's own immune system loses its ability to distinguish ``self'' from ``non-self'' and starts producing antibodies that attack the synovial joints (knees, knuckles, wrists). The fundamental defect is loss of self-tolerance.
Evaluate each statement against the auto-immune mechanism.
(i) ``Ability to differentiate ... increases'' → False. Increased discrimination would prevent auto-immunity. Reject.
(ii) ``Body attacks self cells'' → True. This is the textbook definition of auto-immunity. Accept.
(iii) ``More antibodies are produced'' → Misleading. Quantity of antibodies is not the issue; specificity (against self) is. Reject.
(iv) ``Ability to differentiate ... is lost'' → True. Loss of self-tolerance is the root cause. Accept.
Correct statements: (ii) and (iv). ∴ option (b).
Option (b): ii and iv.
TN
Tara Nair
Ph.D Molecular Biology, NCBS Bangalore
Verified Expert
Strategic angle. Auto-immunity = loss of self/non-self discrimination. Find the two options that say exactly that.
(i) and (iv) are direct opposites; only one can be right. (iv) describes loss of discrimination, which causes RA.
(ii) directly describes self-attack, the consequence.
(iii) is a distractor: more antibodies, not auto-antibodies, would not cause RA.
Option (b).
Cross-check. Cross-check via auto-immunity mechanism. RA, MS, T1DM and SLE all stem from loss of self/non-self discrimination in T-cell selection. Auto-antibodies (e.g. rheumatoid factor for RA) attack synovial joints. Statements (ii) and (iv) capture cause-and-consequence; (i) and (iii) are factually inverted.
Q 7.12
AIDS is caused by HIV. Among the following, which one is not a mode of transmission of HIV?
(a) Transfusion of contaminated blood
(b) Sharing the infected needles
(c) Shaking hands with infected persons
(d) Sexual contact with infected persons
Correct option: (c) Shaking hands with infected persons.
Concept used.HIV is transmitted only through exchange of bodily fluids (blood, semen, vaginal fluid, breast milk). It is not airborne, not transmitted by casual contact (hugging, shaking hands, sharing utensils, mosquito bites), and not transmitted by sweat or tears. Modes of transmission are: unprotected sex, contaminated blood transfusion, sharing of needles, and mother-to-child during pregnancy / delivery / breastfeeding.
Check each option:
(a) blood transfusion → valid mode of transmission.
(b) shared needles → valid mode.
(c) shaking hands → NOT a mode. HIV does not survive on dry skin and there is no fluid exchange.
(d) unprotected sex → valid mode.
The question asks which is not a mode. Hence (c).
Option (c).
IB
Ishaan Banerjee
M.Sc Microbiology, JNU
Verified Expert
Quick reading. The question is negative (``which is not''). Tag each option as ``fluid exchange yes/no''.
Blood transfusion, needle sharing, sexual contact: all involve fluid exchange → valid HIV routes.
Hand-shaking: no fluid exchange → no HIV transmission.
Option (c).
Cross-check. Cross-check via transmission biology. HIV requires fluid exchange — blood, semen, vaginal secretions, breast milk. Casual contact (handshake, hug, shared utensils, mosquito bites, sweat) carries zero documented risk because HIV does not survive on dry skin and there is no fluid breach.
Q 7.13
`Smack' is a drug obtained from the:
(a) latex of Papaver somniferum
(b) leaves of Cannabis sativa
(c) flowers of Dhatura
(d) fruits of Erythroxyl coca
Correct option: (a) Latex of Papaver somniferum.
Concept used.Smack is a street name for heroin (diacetylmorphine), an opioid derived from morphine. Morphine and its derivatives are obtained from the dried latex of the unripe seed-capsules of the opium poppy (Papaver somniferum). The other options are also drug sources, but for different drugs:
Cannabis sativa→ marijuana, hashish, ganja (cannabinoids from inflorescence and resin).
Mnemonic anchor.Smack Sleep (opioid sedation) — Papaver. Cannabis Chill — marijuana/charas. Coca Crash — cocaine. Datura Delirium — atropine. NCERT also notes that diacetyl-morphine (heroin/smack) is a depressant that slows respiration; this is why opioid overdose kills via respiratory depression.
Q 7.14
The substance produced by a cell in viral infection that can protect other cells from further infection is:
(a) serotonin
(b) colostrum
(c) interferon
(d) histamine
Correct option: (c) Interferon.
Concept used.Interferons (IFNs) are antiviral cytokines (small signalling proteins) released by virus-infected cells. They diffuse to neighbouring uninfected cells and bind to specific receptors, triggering those cells to produce antiviral proteins (oligoadenylate synthetase, RNase L, PKR) that block viral replication. Thus interferons set up an antiviral state in the surrounding cells before the virus can reach them.
Reject (a) serotonin: a neurotransmitter; not antiviral.
Reject (b) colostrum: the first milk after birth, rich in IgA antibodies; protects the infant only.
Accept (c) interferon: matches both ``produced by a cell in viral infection'' and ``protects other cells''.
Reject (d) histamine: an inflammatory mediator released in allergies.
Option (c): Interferon.
KG
Krishna Gupta
Ph.D Molecular Biology, NCBS Bangalore
Verified Expert
Strategic angle. The question describes paracrine antiviral signalling. That is the exact biological role of interferon.
Translate the stem: ``signal from one infected cell to nearby cells'' = paracrine signalling.
Among the four, only interferon has this antiviral paracrine role.
Option (c).
Cross-check. Cross-check via cytokine function. Interferon-α/β are released by virus-infected cells, bind IFN receptors on neighbours, and upregulate antiviral enzymes (OAS, PKR, RNase L). Serotonin is a CNS neurotransmitter; colostrum is breast milk's first secretion; histamine drives allergic vasodilation.
Q 7.15
Transplantation of tissues/organs to save certain patients often fails due to rejection of such tissues/organs by the patient. Which type of immune response is responsible for such rejections?
(a) auto-immune response
(b) humoral immune response
(c) physiological immune response
(d) cell-mediated immune response
Concept used. Acquired immunity has two arms. Humoral immunity is antibody-mediated (B-cells → plasma cells → antibodies in blood) and targets extracellular pathogens. Cell-mediated immunity (CMI) is mediated by T-lymphocytes (cytotoxic T-cells, helper T-cells) and targets intracellular pathogens, tumour cells, and grafted/foreign tissues. Graft rejection is driven by cytotoxic T-cells recognising foreign MHC molecules on the donor tissue.
Match the trigger (foreign tissue) to the right arm of immunity. T-cells recognise foreign MHC class I on donor cells. This is cell-mediated.
Reject (a) auto-immune: the patient is not attacking self-tissue here, but foreign tissue.
Reject (b) humoral: antibodies play a smaller role in graft rejection compared to T-cells.
Reject (c) physiological: not a standard immunology term in NCERT.
Accept (d) cell-mediated.
Option (d): Cell-mediated immune response.
MK
Meera Kapoor
Ph.D Molecular Biology, NCBS Bangalore
Verified Expert
Strategic angle. The transplanted tissue is intracellular antigen-rich (cells with foreign MHC). T-cells own this turf.
Antibodies in blood cannot reach intracellular MHC molecules; only T-cells with TCR can read MHC.
Cytotoxic T-cells lyse the graft cells → rejection.
Option (d).
Cross-check. Cross-check via transplant immunology. Donor cells display foreign MHC class I, which cytotoxic T-cells read via TCR + co-receptors. T-cell mediated cytolysis is therefore the rejection mechanism. Humoral antibodies play only a supporting role (hyperacute rejection in pre-sensitised recipients).
Clinical context. To minimise graft rejection, recipients receive (i) HLA-typed donors (closer MHC match = milder rejection), and (ii) life-long immunosuppressants (cyclosporine, tacrolimus, MMF, low-dose steroids) that blunt T-cell activation. Identical-twin transplants are unique in needing no immunosuppression.
Q 7.16
Antibodies present in colostrum which protect the new born from certain diseases is of:
(a) Ig G type
(b) Ig A type
(c) Ig D type
(d) Ig E type
Correct option: (b) IgA type.
Concept used.Colostrum is the yellowish first milk secreted by the mother in the first 2–3 days after delivery. It is rich in secretory IgA (sIgA) antibodies, which coat the infant's gut mucosa and protect against gastrointestinal pathogens. The other classes have different roles: IgG crosses the placenta during pregnancy (not colostrum-related); IgD is a B-cell receptor; IgE mediates allergic responses.
Identify the body fluid: colostrum (breast milk).
Identify the antibody class enriched in mucosal secretions: IgA.
Hence (b).
Option (b): IgA type.
RC
Rohit Chatterjee
M.Sc Biotechnology, AIIMS Delhi
Verified Expert
Mnemonic. IgA = ``A for alimentary'' (gut secretions, milk, saliva, tears). IgG = ``G for gestation'' (placental). IgE = ``E for eosinophil/allergy''. IgM = ``M for first/Mass'' (first to appear).
Colostrum is a gut-bound secretion.
Apply IgA = alimentary mnemonic.
Option (b).
Cross-check. Cross-check via mucosal immunity. Colostrum delivers secretory IgA (sIgA) that coats the infant gut lining and blocks pathogen adhesion. IgG crosses the placenta during pregnancy (not via milk); IgD sits on B-cell surface as a receptor; IgE binds mast cells in allergy.
Q 7.17
Tobacco consumption is known to stimulate secretion of adrenaline and nor-adrenaline. The component causing this could be:
(a) Nicotine
(b) Tannic acid
(c) Curamin
(d) Catechin
Correct option: (a) Nicotine.
Concept used. Tobacco contains over 4000 chemicals. The principal psychoactive and cardiovascular agent is nicotine, an alkaloid that binds nicotinic acetylcholine receptors on chromaffin cells of the adrenal medulla, triggering release of adrenaline (epinephrine) and noradrenaline (norepinephrine). These catecholamines raise blood pressure, heart rate and alertness — the rush smokers feel.
Reject (b) tannic acid: gives tea / tobacco its astringency but is not the catecholamine-stimulating agent.
Reject (c) ``curamin'': curcumin (from turmeric) is unrelated to tobacco.
Reject (d) catechin: a flavonoid found in tea; antioxidant, not catecholamine-stimulating.
Cross-check. Cross-check via receptor pharmacology. Nicotine binds nicotinic acetylcholine receptors on chromaffin cells of the adrenal medulla, triggering catecholamine release. Tannic acid, catechin and turmeric's curcumin are antioxidants/flavonoids with no catecholamine-stimulating action.
Concept used.Antivenom (also called antivenin) is an example of passive immunisation. Horses (or sheep) are first injected with sub-lethal doses of snake venom; their immune systems produce anti-venom antibodies; serum is collected, purified and given to a snake-bite patient. The patient receives ready-made antibodies that neutralise the venom — fast-acting but short-lived.
Compare with active immunisation (vaccines): one receives an attenuated antigen and produces one's own antibodies over weeks.
In a snake-bite emergency, there is no time to wait for the patient's own antibodies. So the patient is given antibodies directly. This is passive.
Strategic angle. A snake-bite victim needs immediate neutralisation. Direct delivery of antibodies is the only fast option.
Active immunity is too slow for an acute envenomation.
Passive transfer of antibodies works in minutes.
Hence antivenom = antibodies.
Option (c).
Cross-check. Cross-check via passive vs active. A snake-bite patient needs neutralisation in minutes; producing one's own antibodies takes weeks. The only way to deliver minute-scale protection is to inject preformed antibodies (raised in horses against the venom) — passive immunisation.
Q 7.19
Which of the following is not a lymphoid tissue?
(a) Spleen
(b) Tonsils
(c) Pancreas
(d) Thymus
Correct option: (c) Pancreas.
Concept used.Lymphoid tissues are organs and tissues where lymphocytes (B-cells, T-cells) are produced, mature, or activated. They are divided into primary lymphoid organs (bone marrow, thymus — sites of lymphocyte production and maturation) and secondary lymphoid organs (spleen, lymph nodes, tonsils, Peyer's patches, appendix — sites where lymphocytes encounter antigens). The pancreas is a digestive and endocrine organ (produces insulin, glucagon, digestive enzymes), not a lymphoid organ.
Classify each option:
Spleen → secondary lymphoid organ.
Tonsils → secondary lymphoid organ.
Pancreas → digestive + endocrine. NOT lymphoid.
Thymus → primary lymphoid organ (T-cell maturation).
The odd one out is pancreas. Hence (c).
Option (c): Pancreas.
AR
Aditi Rao
M.Sc Microbiology, JNU
Verified Expert
Quick reading. Spleen, tonsils and thymus are textbook lymphoid; pancreas is digestive/endocrine.
Tag each option as lymphoid (L) or non-lymphoid (N).
Spleen L, Tonsils L, Pancreas N, Thymus L.
One N stands out: pancreas.
Option (c).
Cross-check. Cross-check via NCERT 8.3. Lymphoid organs are dedicated to lymphocyte production, maturation or activation. Bone marrow + thymus (primary), spleen + lymph nodes + tonsils + Peyer's patches + appendix (secondary). Pancreas is a digestive (acini) + endocrine (islets) organ — never lymphoid.
Q 7.20
Which of the following glands is large sized at birth but reduces in size with ageing?
(a) Pineal
(b) Pituitary
(c) Thymus
(d) Thyroid
Correct option: (c) Thymus.
Concept used. The thymus is a bilobed gland located near the heart and behind the sternum. It is the site of T-cell maturation. It is maximally active at birth and reaches its largest relative size in childhood. With age (especially after puberty) it undergoes thymic involution — its lymphoid tissue is gradually replaced by adipose tissue, and the gland shrinks dramatically. This is one reason elderly individuals mount weaker T-cell responses to new antigens.
Reject (a) pineal: small at all ages.
Reject (b) pituitary: roughly constant in size through adulthood.
Accept (c) thymus: classic involution gland.
Reject (d) thyroid: typically grows slightly with age.
Option (c): Thymus.
SI
Siddharth Iyer
M.Sc Biotechnology, AIIMS Delhi
Verified Expert
Strategic angle. The unusual property is ``shrinks with age''. Only one gland in the body is famous for shrinking.
Pituitary, thyroid, pineal: roughly constant through adult life.
Thymus: peaks in childhood, then atrophies.
Option (c).
Cross-check. Cross-check via thymic involution. The thymus peaks in childhood and shrinks dramatically after puberty — its lymphoid tissue is replaced by adipose. This explains weaker vaccine responses in the elderly. Pituitary, pineal and thyroid all remain roughly constant in adulthood.
Q 7.21
Haemozoin is a:
(a) precursor of hemoglobin
(b) toxin released from Streptococcus infected cells
(c) toxin released from Plasmodium infected cells
(d) toxin released from Haemophilus infected cells
Correct option: (c) Toxin released from Plasmodium-infected cells.
Concept used.Haemozoin is a dark-brown crystalline pigment produced when Plasmodium (the malarial parasite) digests host haemoglobin inside red blood cells. Haem released from haemoglobin is toxic to the parasite, so the parasite polymerises haem into the inert haemozoin crystal. When the infected RBC ruptures, haemozoin and other parasite products spill into the bloodstream and cause the recurrent cycle of chills, high fever and shivering characteristic of malaria.
Reject (a) precursor of haemoglobin: haemozoin is a breakdown product, not a precursor.
Reject (b) and (d): no association with Streptococcus or Haemophilus.
Accept (c): released by Plasmodium-infected RBCs at rupture.
Option (c).
PR
Pooja Reddy
Ph.D Molecular Biology, NCBS Bangalore
Verified Expert
Strategic angle. The Greek prefix haemo- (blood) hints at RBC connection. The parasite that lives inside RBCs and digests haemoglobin is Plasmodium.
Connect ``haemozoin'' to ``haemoglobin breakdown''.
The only parasite among options that lives inside RBCs is Plasmodium.
Option (c).
Cross-check. Cross-check via malaria pathology. Plasmodium digests host haemoglobin, releasing toxic haem; the parasite polymerises it into inert haemozoin crystals. When RBCs synchronously rupture every 48–72 hours, haemozoin + merozoites spill into blood and trigger the chills-fever-sweat cycle.
Q 7.22
Which of the following is not the causal organism for ringworm?
(a) Microsporum
(b) Trichophyton
(c) Epidermophyton
(d) Macrosporum
Correct option: (d)Macrosporum.
Concept used.Ringworm (tinea, dermatophytosis) is a superficial fungal infection of the skin, hair and nails. It is caused by three dermatophyte genera: Microsporum, Trichophyton, and Epidermophyton. ``Macrosporum'' is not a recognised genus of dermatophytes and is a distractor.
NCERT lists three causal genera: Microsporum, Trichophyton, Epidermophyton.
Match against options. (a), (b), (c) all match. (d) Macrosporum does not.
Hence the ``not'' option is (d).
Option (d): Macrosporum.
NV
Neha Verma
M.Sc Biotechnology, AIIMS Delhi
Verified Expert
Quick reading. Three of the four options are NCERT-listed dermatophytes; the fourth is invented.
Cross-check. Cross-check via fungal taxonomy. Dermatophyte trio for ringworm: Microsporum (hair/skin), Trichophyton (skin/nails), Epidermophyton (skin). ``Macrosporum'' is a fabricated distractor playing on the Micro/Macro prefix swap.
Q 7.23
A person with sickle cell anemia is:
(a) more prone to malaria
(b) more prone to typhoid
(c) less prone to malaria
(d) less prone to typhoid
Correct option: (c) Less prone to malaria.
Concept used.Sickle cell anaemia is a recessive blood disorder caused by a point mutation (Glu → Val at position 6) in the β-globin gene. Heterozygotes (HbA HbS) carry one copy of the mutant allele; their RBCs sickle slightly under low oxygen. Crucially, the malarial parasite Plasmodium falciparum cannot complete its life cycle inside such RBCs — the deformed cells are cleared too quickly by the spleen. As a result, sickle-cell carriers (and to some extent homozygotes who survive to adulthood) are less susceptible to falciparum malaria. This is a classic example of balanced polymorphism or heterozygote advantage: the sickle allele persists at high frequency in African and Indian populations because it protects against malaria.
Recall that the sickle allele's high frequency in Africa overlaps the malarial belt. This is not coincidence.
Plasmodium growth is impaired in sickle-shaped (or sickleable) RBCs.
Hence sickle-cell carriers are less prone to malaria. Reject (a). Accept (c).
No analogous protection exists against typhoid (a bacterial gut infection), so (b) and (d) are irrelevant.
Option (c): Less prone to malaria.
DN
Dev Nair
Ph.D Molecular Biology, NCBS Bangalore
Verified Expert
Strategic angle. If the sickle allele had no benefit, natural selection would have driven it to extinction long ago. Yet it persists — there must be an advantage. That advantage is malaria resistance.
Recall heterozygote advantage = the heterozygote has higher fitness than either homozygote in malaria-endemic regions.
The advantage is protection against Plasmodium.
Hence sickle-cell carriers are less prone to malaria.
Option (c).
Cross-check. Cross-check via heterozygote advantage. Carriers (HbAHbS) have RBCs that sickle when invaded by Plasmodium falciparum and are cleared too quickly by the spleen for the parasite to complete schizogony. The allele's geographic frequency in Africa/India tracks the malaria belt — Darwinian selection at work.
Numerical anchor. In Sub-Saharan Africa, the HbS allele reaches frequencies of 10–20% — far above what mutation alone could maintain. The malaria-mortality differential between HbA HbA and HbA HbS children explains the gap. India's tribal Gond/Bhil populations show similar patterns. Without malaria pressure, the allele would have been purged within ∼ 30 generations.
Very Short Answer Type Questions (VSA)
Q 7.24
Certain pathogens are tissue/organ specific. Justify the statement with suitable examples.
Concept used. Pathogens display tissue tropism — a preference for invading a particular tissue, organ or cell type. This specificity arises because the pathogen requires particular host surface receptors, intracellular machinery, or microenvironmental conditions found only in that tissue.
State the claim: many pathogens enter the body through a general route (mouth, lungs, blood) but multiply only in a specific organ.
Give worked examples of tropism.
Plasmodium (malaria) sporozoites enter through a mosquito bite but multiply only in liver cells and then RBCs, because these cells have the receptors and the haemoglobin the parasite needs.
Mycobacterium tuberculosis preferentially infects the lungs (and sometimes lymph nodes, bones, kidneys).
Wuchereria (filaria) lodges in lymphatic vessels of the lower limbs.
HIV specifically infects CD4+ T-helper cells.
Salmonella typhi targets the small intestine and then the gallbladder.
Conclude: pathogen specificity is the rule, not the exception.
Pathogens are tissue/organ specific because they need particular host receptors and microenvironment; e.g. HIV → CD4 T-cells, Plasmodium→ liver & RBC, filaria → lymphatic vessels.
IJ
Ishita Joshi
M.Sc Biotechnology, AIIMS Delhi
Verified Expert
Strategic angle. Frame the answer in two parts: (1) why specificity exists (receptors / niche), (2) two crisp examples.
Mechanism: pathogen surface proteins recognise a specific host receptor, which is expressed on only one tissue. No receptor = no entry = no infection.
Example 1: HIV's gp120 binds CD4 + CCR5/CXCR4, both displayed on T-helper cells, so HIV targets them.
Example 2: Plasmodium merozoite proteins bind glycophorin on RBCs.
Cross-check. Cross-check via receptor biology. HIV gp120 binds CD4 + co-receptor (CCR5/CXCR4) — only T-helper cells, macrophages and dendritic cells display this combination. Plasmodium merozoites bind glycophorin on RBCs. S. typhi invades intestinal M-cells. Same logic, different receptor-tissue pair each time.
Q 7.25
The immune system of a person is suppressed. In the ELISA test, he was found positive to a pathogen.
(a) Name the disease the patient is suffering from.
(b) What is the causative organism?
(c) Which cells of body are affected by the pathogen?
Concept used.ELISA (Enzyme-Linked Immunosorbent Assay) is the standard antibody-based test for HIV diagnosis. A positive ELISA combined with immune suppression points to AIDS (Acquired Immuno-Deficiency Syndrome), caused by the Human Immunodeficiency Virus (HIV). HIV preferentially infects and destroys helper T-lymphocytes (CD4+ T-cells), which orchestrate the entire acquired immune response. Their depletion is what produces the immune-suppressed phenotype.
(a) The disease is AIDS.
(b) The causative organism is HIV (Human Immunodeficiency Virus), a retrovirus of the family Retroviridae.
(c) HIV infects helper T-lymphocytes (CD4+ T-cells) and, to a lesser extent, macrophages and dendritic cells.
(a) AIDS; (b) HIV (a retrovirus); (c) helper T-lymphocytes (CD4+ T-cells).
AK
Aarav Kapoor
Ph.D Molecular Biology, NCBS Bangalore
Verified Expert
Quick reading. Two clues: ``immune system suppressed'' + ``ELISA positive''. These two together name AIDS uniquely.
Map ``ELISA positive'' → HIV antibodies present.
Map ``immune suppressed'' → AIDS phase, not just HIV carrier.
HIV destroys CD4 T-cells → loss of helper signal → both humoral and cell-mediated arms collapse.
Cross-check. Cross-check via NCERT line. Chapter 8 opens with: ``Health does not simply mean `absence of disease' or `physical fitness'; it is a state of complete physical, mental and social well-being.'' Options (a),(b),(d) each capture a fragment (mind/body, mood, economics) but only (c) reproduces the full WHO triad — the verbatim Class 12 NCERT definition.
Where are B-cells and T-cells formed? How do they differ from each other?
Concept used. Both B-lymphocytes and T-lymphocytes are formed in the bone marrow from a common haematopoietic stem cell. They diverge by site of maturation: B-cells mature in the bone marrow itself, while T-cells migrate to and mature in the thymus.
State formation sites: B-cells → bone marrow (formation + maturation). T-cells → bone marrow (formation) and thymus (maturation).
State functional differences:
B-cells mediate humoral immunity by secreting antibodies (immunoglobulins) against extracellular pathogens.
T-cells mediate cell-mediated immunity by directly killing infected cells (cytotoxic T) or by helping B-cells and macrophages (helper T).
Both formed in bone marrow; B-cells mature in bone marrow and secrete antibodies; T-cells mature in thymus and mediate cell-mediated immunity.
PS
Priya Singh
M.Sc Microbiology, JNU
Verified Expert
Strategic angle. A two-column compare/contrast covers this question cleanly.
B-cell origin and maturation: bone marrow. T-cell origin: bone marrow; T-cell maturation: thymus.
Recognise antigen differently: B-cells via membrane-bound antibody (BCR); T-cells via T-cell receptor reading MHC-presented peptides.
Cross-check. Cross-check via etymology. Pathogen = pathos (suffering) + genes (producer), so a pathogen causes disease by definition. Vectors merely transport pathogens (Anopheles for Plasmodium, Culex for Wuchereria, Aedes for Dengue/Chikungunya). Insects and worms are taxonomic groups, not functional disease-causer labels.
Both born in bone marrow; B matures in bone marrow → antibodies; T matures in thymus → cell-mediated.
Q 7.27
Given below are the pairs of pathogens and the diseases caused by them. Which out of these is not a matching pair and why?
(a) Virus common cold
(b) Salmonella typhoid
(c) Microsporum filariasis
(d) Plasmodium malaria
Concept used. Each disease has a specific causative organism. Filariasis is caused by the helminth Wuchereria (or Brugia), not by Microsporum, which is one of the fungi that cause ringworm.
Verify each pair.
(a) Virus (rhinovirus) → common cold. Correct.
(b) Salmonella typhi→ typhoid. Correct.
(c) Microsporum→ ringworm, not filariasis. Wrong pair.
(d) Plasmodium→ malaria. Correct.
The mismatched pair is (c). The correct cause of filariasis is Wuchereria bancrofti / Wuchereria malayi.
Mismatched pair: (c) Microsporum filariasis. Microsporum causes ringworm; filariasis is caused by Wuchereria.
KM
Kavya Mehta
M.Sc Biotechnology, AIIMS Delhi
Verified Expert
Strategic angle. The fastest way is to recall the cause of each option's disease and tag matches.
Common cold → rhinovirus. Match.
Typhoid →Salmonella typhi. Match.
Filariasis →Wuchereria, not Microsporum. Mismatch.
Malaria →Plasmodium. Match.
Cross-check. Cross-check via diagnostic principle. Widal exploits agglutination of the patient's anti-Salmonella antibodies with O and H antigens of S. typhi. ELISA targets HIV antibodies; ESR is a non-specific inflammatory marker; PCR amplifies nucleic acids. Only Widal is antigen-specific for typhoid.
(c) is the mismatch.
Q 7.28
What would happen to immune system, if thymus gland is removed from the body of a person?
Concept used. The thymus is the primary lymphoid organ where T-lymphocytes mature. Removal of the thymus (thymectomy), especially in early life, prevents the development of mature T-cells.
Without thymus → no T-cell maturation → no functional T-cells.
Consequences for the immune system:
Loss of cell-mediated immunity: cytotoxic T-cells cannot kill infected cells; intracellular pathogens (viruses, Mycobacterium) cannot be cleared.
Loss of T-helper signals: B-cells receive no help, so antibody production against most antigens collapses.
Severely weakened response to grafts (failure to reject) and to tumour surveillance.
The person becomes severely immune-compromised, similar to a SCID phenotype.
Removal of thymus halts T-cell maturation; cell-mediated immunity is lost, and antibody responses (which need T-cell help) are sharply weakened.
SB
Sneha Bhat
M.Sc Microbiology, JNU
Verified Expert
Quick reading. No thymus → no mature T-cells → both arms of acquired immunity hobbled.
Antibody quantity drops sharply because B-cells need helper T-cell signals.
Cross-check. Cross-check via classification rule. Infectious = caused by a transmissible pathogen. Influenza (orthomyxovirus, droplet) and small-pox (Variola, contact/droplet) tick both boxes. Cancer arises from accumulated mutations; allergies are IgE hypersensitivities to harmless antigens — neither requires a pathogen or person-to-person transmission.
Severe immunodeficiency from loss of T-cells; both cell-mediated immunity and antibody responses fail.
Q 7.29
Many microbial pathogens enter the gut of humans along with food. What are the preventive barriers to protect the body from such pathogens? What type of immunity do you observe in this case?
Concept used. The body has several layered innate immunity barriers that prevent ingested pathogens from establishing infection. Innate immunity is non-specific, present from birth, and forms the first line of defense.
Identify the gut-specific barriers:
Saliva in the mouth contains lysozyme that breaks bacterial cell walls.
Gastric HCl in the stomach kills most ingested microbes by extreme acidity (pH ≈ 1.5–2).
Mucus lining the gut traps microbes.
Resident gut microflora competitively exclude pathogens.
Peyer's patches and gut-associated lymphoid tissue (GALT) mount localised IgA responses.
Classify the immunity. These barriers (saliva, mucus, HCl, normal flora) are innate (non-specific) immunity — specifically the physiological + cellular barriers.
Cross-check. Cross-check via NCERT figure 8.2. The diagram explicitly traces: gametocytes ingested → fertilisation in mosquito gut → zygote → oocyst on gut wall → sporozoites → migrate to salivary glands → injected on next bite. NCERT labels the salivary-gland sporozoites as the infective stage.
Why is mother's milk considered the most appropriate food for a new born infant?
Concept used. Breast milk is uniquely matched to infant nutritional and immune needs. The first secretion (colostrum, in the first 2–3 days) is exceptionally rich in immunoglobulins, especially secretory IgA, which coats the infant's gut.
List nutritional benefits: balanced proteins, fats, lactose, vitamins, minerals, water — all at the right concentration and temperature; easy to digest.
List immune benefits:
Antibodies: colostrum is rich in IgA, which protects against gut infections.
Lactoferrin, lysozyme, oligosaccharides provide additional antimicrobial defence.
Confers passive natural immunity until the baby's own immune system matures.
Other benefits: promotes bonding; sterile and at body temperature.
Mother's milk (especially colostrum) provides complete nutrition plus IgA antibodies that confer passive immunity to the newborn.
DC
Diya Chatterjee
M.Sc Microbiology, JNU
Verified Expert
Quick reading. Two reasons: nutrition + immunity. Nutrition because the composition is matched to infant digestion; immunity because of maternal IgA.
Nutritional fit: protein/fat/carb balance; high digestibility.
Passive immunity: IgA in colostrum coats infant gut and protects against pathogens for first months.
Cross-check. Cross-check via vector–disease table. Aedes aegypti day-biter transmits dengue, chikungunya, yellow fever, Zika. Anopheles (night-biter) carries Plasmodium; Culex carries Wuchereria. House flies and cockroaches contaminate food mechanically but are not biological vectors for chikungunya virus.
Best food: complete nutrition + maternal IgA giving passive immunity.
Q 7.31
What are interferons? How do interferons check infection of new cells?
Concept used.Interferons (IFNs) are antiviral cytokines — small signalling proteins released by virus-infected cells. They are part of the body's innate immunity response and act in a paracrine (cell-to-cell) manner.
Definition: Interferons are glycoproteins secreted by virus-infected cells.
Cross-check. Cross-check via pathology. Pneumonia consolidates alveoli with neutrophilic exudate, so the symptoms cluster around impaired gas exchange: cough, fever, chills, dyspnea, and (in severe cases) cyanosis of lips and finger-tips. Abdominal symptoms point to typhoid or amoebiasis, not pneumonia.
IFNs are antiviral cytokines that put neighbour cells in an antiviral state, halting viral spread.
Q 7.32
In the figure, structure of an antibody molecule is shown. Name the parts A, B and C. Show A, B and C in the diagram.
Concept used. A typical antibody (immunoglobulin) has the formula H2 L2 — two identical heavy (H) chains and two identical light (L) chains, joined together by disulphide bonds into a Y-shape. The arms of the Y have variable regions that form the antigen-binding sites. The labels typically asked in this diagram are: A = antigen, B = light chain, C = heavy chain. Some versions of the figure label A = antigen-binding site, B = light chain, C = heavy chain.
Fig. 8.1 (NCERT Exemplar Class 12 Biology Chapter 8): antibody molecule with two heavy chains, two light chains, two antigen-binding sites and inter-chain disulphide bridges.
Identify the Y-shape: top two arms = Fab regions (variable); base = Fc region (constant).
Identify A, B, C from typical NCERT labelling.
A = Antigen-binding site (top of each arm).
B = Light chain (the shorter polypeptide flanking each arm).
C = Heavy chain (the longer polypeptide running through each arm and into the stem).
Note: the molecule is held together by inter-chain disulphide (S–S) bridges (visible in the figure).
A = antigen-binding site; B = light chain; C = heavy chain.
AB
Aaditya Banerjee
M.Sc Biotechnology, AIIMS Delhi
Verified Expert
Picture-first. The Y-shape's top tips are the working ends (antigen-binding); the long chains are H; the short chains are L.
Top tip (A) = antigen-binding site.
Short outer chain (B) = light chain.
Long central chain (C) = heavy chain.
Cross-check. Cross-check via Greek roots. Onkos = mass/tumour, so any -gene with the onko- root is by construction a cancer-causing gene. Structural/expressor/regulatory genes are generic categories. Crucially, oncogenes arise from mutated proto-oncogenes — the same gene family that normally controls the cell cycle.
A: antigen-binding site; B: light chain; C: heavy chain.
Antibody class table. IgG (most abundant, crosses placenta), IgA (mucosal/colostrum, dimeric), IgM (largest pentameric, first responder), IgE (allergy + parasites, mast-cell binding), IgD (B-cell surface receptor). The H2 L2 tetramer is the same in all five — only the heavy-chain constant region differs (Fc).
Q 7.33
If a regular dose of drug or alcohol is not provided to an addicted person, he shows some withdrawal symptoms. List any four such withdrawal symptoms.
Concept used.Addiction produces physical dependence: the body adapts to the constant presence of the drug, and its sudden absence triggers a stereotyped set of withdrawal symptoms (also called abstinence syndrome).
Recall the classical withdrawal-symptom list.
Anxiety, restlessness and irritability.
Shakiness or tremors.
Nausea, vomiting and sweating.
Strong craving for the drug; depression; insomnia.
Any four of the above are acceptable. Severe alcohol withdrawal can also cause seizures and hallucinations.
Four withdrawal symptoms: anxiety, tremors / shaking, nausea & sweating, strong craving for the substance.
PD
Pooja Desai
M.Sc Microbiology, JNU
Verified Expert
Quick reading. Withdrawal = body's protest at the missing dose. Pick four symptoms that span CNS and autonomic systems.
CNS: anxiety, irritability, insomnia.
Autonomic: sweating, tremors, palpitations.
GI: nausea, vomiting.
Craving for the drug.
Cross-check. Cross-check via hallmark definition. The defining property of malignancy is ability to invade adjacent tissue and seed secondary tumours via blood/lymph — i.e. metastasis. Mitosis is a normal universal process; metagenesis is alternation of generations (Obelia); teratogenesis is birth-defect biology.
Anxiety, tremors, nausea, craving.
Q 7.34
Why is it that during changing weather, one is advised to avoid closed, crowded and airconditioned places like cinema halls etc.?
Concept used. Many respiratory pathogens (rhinovirus, influenza, Streptococcus pneumoniae, Haemophilus influenzae) spread by airborne droplet transmission. Closed, crowded, air-conditioned spaces re-circulate the same air, increasing pathogen load and increasing person-to-person transmission.
During changing weather, body's mucosal defences are stressed (cold air dries mucus), and many pathogens flourish (rhino-, influenza viruses).
Result: a single infectious person can infect many others quickly.
Avoiding such places reduces exposure and disease incidence.
Closed, crowded, AC spaces concentrate respiratory pathogens in re-circulated air; one infected person spreads to many. Hence avoid them during seasonal transitions.
KI
Karan Iyer
M.Sc Microbiology, JNU
Verified Expert
Strategic angle. Probability-of-exposure framing.
Number of pathogenic droplets per cubic metre is higher when (a) many people exhale, (b) air does not circulate fresh outdoor air.
AC + closed + crowded → maximum droplets per breath.
Hence higher chance of infection.
Cross-check. Cross-check via WHO triad. A psychiatrist evaluates the mental + social pillars. ``Apparently healthy'' rules out physical illness; ``unhealthy by psychiatrist'' must therefore reflect dysfunction in mood, cognition, behaviour or social adjustment. Work-efficiency, income and sporting hobbies are not WHO health pillars.
High pathogen density in re-circulated air means higher infection risk.
Q 7.35
The harmful allele of sickle cell anemia has not been eliminated from human population. Such afflicted people derive some other benefit. Discuss.
Concept used. The sickle-cell allele (HbS) is maintained in malaria-endemic populations by heterozygote advantage (balanced polymorphism). Heterozygotes (HbA HbS) are resistant to falciparum malaria because their RBCs sickle when invaded by Plasmodium, leading to rapid clearance of infected cells by the spleen.
In malaria-endemic Africa and India, HbA HbA homozygotes are susceptible to fatal malaria.
HbS HbS homozygotes have severe anaemia and die young, so this genotype is at a disadvantage.
HbA HbS heterozygotes have only mild anaemia but strong malaria resistance; they survive and reproduce best.
Natural selection therefore maintains the HbS allele at intermediate frequency: the death toll from sickle disease is balanced by the survival advantage during malaria epidemics. This is balanced polymorphism.
Sickle cell allele persists because heterozygotes are protected from falciparum malaria — a classic heterozygote advantage.
TM
Tara Mehta
Ph.D Molecular Biology, NCBS Bangalore
Verified Expert
Strategic angle. A harmful allele persists only if it confers fitness in some genotype. Find that genotype.
HbS HbS = disease, low fitness.
HbA HbA = no protection from malaria, dies in epidemics.
Cross-check. Cross-check via auto-immunity mechanism. RA, MS, T1DM and SLE all stem from loss of self/non-self discrimination in T-cell selection. Auto-antibodies (e.g. rheumatoid factor for RA) attack synovial joints. Statements (ii) and (iv) capture cause-and-consequence; (i) and (iii) are factually inverted.
Heterozygote (HbA HbS) is protected against malaria, so the sickle allele is maintained by balanced polymorphism.
Q 7.36
Lymph nodes are secondary lymphoid organs. Explain the role of lymph nodes in our immune response.
Concept used.Lymph nodes are small bean-shaped organs scattered along lymphatic vessels. They serve as filtration stations and meeting points where antigens carried by lymph encounter lymphocytes, triggering specific immune responses.
Filtration: lymph from tissues enters the node, where macrophages remove microbes, debris and cancer cells.
Antigen presentation: dendritic cells in the node display antigen fragments to lymphocytes.
Lymphocyte activation: B-cells and T-cells encounter their cognate antigen, become activated, proliferate (clonal expansion) and differentiate into effector cells.
Antibody production: activated B-cells become plasma cells that pour antibodies into the lymph and blood.
Memory formation: some activated cells become memory cells, providing rapid recall response on future exposure.
Lymph nodes filter lymph, present antigens, activate B & T-cells, produce antibodies, and generate memory cells — they are the principal sites where adaptive immune responses are mounted.
NV
Nikhil Verma
M.Sc Biotechnology, AIIMS Delhi
Verified Expert
Picture-first. Lymph nodes are airport-style hubs: lymph carrying antigen lands there; lymphocytes already in the hub catch the antigen and ``board''.
Antigens in lymph reach the node.
Lymphocytes patrolling the node encounter their specific antigen.
Clonal selection, proliferation, antibody production follow.
Cross-check. Cross-check via transmission biology. HIV requires fluid exchange — blood, semen, vaginal secretions, breast milk. Casual contact (handshake, hug, shared utensils, mosquito bites, sweat) carries zero documented risk because HIV does not survive on dry skin and there is no fluid breach.
Lymph nodes are the meeting hubs where antigens activate B and T-cells, generating adaptive immunity and memory.
Q 7.37
Why is an antibody molecule represented as H2 L2?
Concept used. A typical antibody (immunoglobulin) is a tetramer of four polypeptide chains: two identical heavy (H) chains and two identical light (L) chains, linked by disulphide bonds into a Y-shape.
Count the chains: 2 heavy + 2 light = 4 polypeptide chains in total.
Express stoichiometrically: H× 2 + L× 2 = H2 L2.
Therefore the formula representation is H2 L2.
An antibody has 2 heavy + 2 light chains, hence the formula H2 L2.
AJ
Aanya Joshi
M.Sc Microbiology, JNU
Verified Expert
Strategic angle. The notation is purely a chain-count formula.
What does the term `memory' of the Immune system mean?
Concept used.Immunological memory is the ability of the acquired immune system to mount a faster, larger and more specific response on second (or later) exposure to the same antigen than on the first exposure. The cells responsible are memory B-cells and memory T-cells formed during the primary response.
During the first exposure, some activated B and T-cells differentiate not into short-lived effectors but into long-lived memory cells that persist for years to decades.
On re-exposure, these memory cells recognise the antigen immediately, proliferate rapidly, and generate plasma cells / cytotoxic cells in days rather than weeks.
This secondary response produces high-affinity IgG antibodies in large amounts, often clearing the pathogen before symptoms appear.
Vaccination relies on this memory: a vaccine creates memory cells without the danger of the disease.
Immune memory = the ability to recognise a previously-encountered antigen and mount a faster, stronger response, mediated by long-lived memory B and T-cells.
RR
Riya Rao
Ph.D Molecular Biology, NCBS Bangalore
Verified Expert
Quick reading. First contact = slow, weak primary response. Second contact = fast, strong secondary response. The difference is memory.
Primary response peaks at 2–3 weeks, IgM dominant.
Secondary response peaks in days, IgG dominant, much higher titre.
Memory B + memory T cells make this possible.
Cross-check. Cross-check via cytokine function. Interferon-α/β are released by virus-infected cells, bind IFN receptors on neighbours, and upregulate antiviral enzymes (OAS, PKR, RNase L). Serotonin is a CNS neurotransmitter; colostrum is breast milk's first secretion; histamine drives allergic vasodilation.
Memory = faster and stronger second-time response due to long-lived memory lymphocytes.
Q 7.39
If a patient is advised Anti Retroviral Therapy, which infection is he suffering from? Name the causative organism.
Concept used.Anti-Retroviral Therapy (ART) is a combination drug regimen (typically 3 or more drugs from different classes) that suppresses the replication of retroviruses, especially HIV.
Identify infection: ART is the standard treatment for AIDS / HIV infection.
Identify pathogen: the causative organism is the Human Immunodeficiency Virus (HIV), a retrovirus belonging to the family Retroviridae.
Why ``retroviral''? HIV stores its genome as RNA and uses reverse transcriptase to copy RNA → DNA inside the host cell. Drugs target this enzyme (NRTIs, NNRTIs), the integrase, or the protease.
The patient has HIV / AIDS infection; the causative organism is the Human Immunodeficiency Virus (HIV), a retrovirus.
YP
Yash Patel
M.Sc Biotechnology, AIIMS Delhi
Verified Expert
Quick reading. ``Anti-Retroviral'' names the target: retroviruses. The only human retroviral disease in the NCERT syllabus is HIV/AIDS.
Drug class name → retrovirus.
Retrovirus in NCERT → HIV.
Disease → AIDS.
Cross-check. Cross-check via transplant immunology. Donor cells display foreign MHC class I, which cytotoxic T-cells read via TCR + co-receptors. T-cell mediated cytolysis is therefore the rejection mechanism. Humoral antibodies play only a supporting role (hyperacute rejection in pre-sensitised recipients).
HIV / AIDS, caused by Human Immunodeficiency Virus (retrovirus).
Short Answer Type Questions (SA)
Q 7.40
Differentiate between active immunity and passive immunity.
Concept used.Active immunity is generated when the host's own immune system encounters an antigen (natural infection or vaccine) and produces specific antibodies and memory cells. Passive immunity is conferred when preformed antibodies (from another source) are introduced into the host; the host's immune system does not learn or remember.
State origin: active = host's own response; passive = ready-made antibodies given.
Onset and duration: active is slow to develop (1–2 weeks) but long-lasting (often life-long) due to memory cells; passive is immediate but short-lived (a few weeks) because the antibodies are not replenished.
Examples:
Active natural: recovery from chickenpox.
Active artificial: vaccination (DPT, MMR).
Passive natural: maternal IgG via placenta; IgA via colostrum.
Memory: active immunity generates memory; passive does not.
Active immunity: host's own response, slow onset, long-lasting, has memory (e.g. vaccines). Passive immunity: preformed antibodies given, immediate but short-lived, no memory (e.g. antivenom).
AS
Aanya Singh
M.Sc Biotechnology, AIIMS Delhi
Verified Expert
Strategic angle. A tabular comparison covers every NCERT-test marker in one block.
Origin: own vs. external.
Speed of protection: weeks vs. minutes.
Duration: long vs. short.
Memory: yes vs. no.
Examples: vaccine vs. antivenom.
Cross-check. Cross-check via mucosal immunity. Colostrum delivers secretory IgA (sIgA) that coats the infant gut lining and blocks pathogen adhesion. IgG crosses the placenta during pregnancy (not via milk); IgD sits on B-cell surface as a receptor; IgE binds mast cells in allergy.
Diagnostic angle. On histology, malignant cells show pleomorphism (variable cell shape), hyperchromatic nuclei, abnormal mitoses (tripolar spindles) and loss of architecture. Benign tumours look like their tissue of origin (well-differentiated). Pathologists also grade malignancy (I–IV) by extent of differentiation.
Q 7.41
Differentiate between benign tumor and malignant tumor.
Concept used. Tumours are classified by their growth behaviour. A benign tumour is non-cancerous, encapsulated, slow-growing, and confined to the site of origin. A malignant tumour is cancerous: it grows rapidly, invades surrounding tissue, and metastasises to distant organs via blood and lymph.
Growth rate: benign = slow; malignant = rapid and uncontrolled.
Capsule: benign tumours are usually encapsulated; malignant tumours have ill-defined borders and infiltrate adjacent tissue.
Metastasis: benign tumours stay where they form; malignant tumours seed secondary tumours at distant sites.
Risk to life: benign tumours rarely kill (unless they compress a vital organ); malignant tumours are often fatal if untreated.
Cell appearance: benign cells resemble the tissue of origin (well-differentiated); malignant cells are poorly differentiated and often have abnormal nuclei.
Benign: slow, encapsulated, non-invasive, no metastasis, rarely fatal. Malignant: rapid, invasive, metastasises, often fatal — true cancer.
KR
Karan Reddy
Ph.D Molecular Biology, NCBS Bangalore
Verified Expert
Quick reading. Capsule + metastasis are the two NCERT-tested differences.
Benign → encapsulated → surgeon removes it whole → cure.
Malignant → no capsule → infiltrates + metastasises → needs chemo / radio / surgery in combination.
Cross-check. Cross-check via receptor pharmacology. Nicotine binds nicotinic acetylcholine receptors on chromaffin cells of the adrenal medulla, triggering catecholamine release. Tannic acid, catechin and turmeric's curcumin are antioxidants/flavonoids with no catecholamine-stimulating action.
Benign: encapsulated, no spread. Malignant: invasive, metastases.
Epidemiology. The WHO estimates passive smoke kills ∼ 1.2 million non-smokers annually worldwide, half of them children. The fraction of homes with smokers correlates with childhood asthma, bronchitis and SIDS. Indian Tobacco-Free Workplace rules ban smoking in public spaces precisely to protect passive smokers.
Q 7.42
Do you consider passive smoking is more dangerous than active smoking? Why?
Concept used.Passive (second-hand) smoking is inhaling the smoke exhaled by a smoker or smoke from a burning cigarette. Side-stream smoke (from the cigarette tip) is unfiltered and contains higher concentrations of certain carcinogens (carbon monoxide, nicotine, tar, benzopyrene) per gram than the mainstream smoke a smoker inhales through the filter.
Composition difference: side-stream smoke from the lit end of a cigarette burns at a lower temperature than the smoker's puff, producing more carcinogens (benzopyrenes, nitrosamines).
Lack of filter: smokers' filters trap a fraction of particulates and tar; passive smokers receive un-filtered smoke directly.
Vulnerable victims: children and pregnant women are common passive smokers; they cannot choose to leave the environment, magnifying risk.
Result: passive smokers can develop the same diseases as active smokers — lung cancer, COPD, cardiovascular disease — without ever choosing to smoke. In that sense, passive smoking is more dangerous or at least as dangerous: the victim has no agency, the smoke is unfiltered, and side-stream smoke is chemically harsher.
Yes, passive smoking can be more dangerous: side-stream smoke is unfiltered and richer in carcinogens, and passive smokers (often children, pregnant women) inhale it involuntarily.
AV
Aditya Verma
M.Sc Microbiology, JNU
Verified Expert
Strategic angle. Three reasons that make passive smoking dangerous: (i) unfiltered side-stream smoke, (ii) involuntary exposure, (iii) vulnerable victims.
Side-stream smoke is richer in carbon monoxide, ammonia, formaldehyde than mainstream smoke.
Children of smokers have higher rates of asthma, ear infections, and SIDS.
Pregnant non-smokers exposed to passive smoke have higher rates of low birth weight.
Cross-check. Cross-check via passive vs active. A snake-bite patient needs neutralisation in minutes; producing one's own antibodies takes weeks. The only way to deliver minute-scale protection is to inject preformed antibodies (raised in horses against the venom) — passive immunisation.
Passive smoking is comparable or worse: unfiltered, richer carcinogens, involuntary exposure.
Cost-effectiveness anchor. A polio dose costs < 0.20; treating a paralytic case costs lifetime medical care + lost productivity in the lakhs. Smallpox vaccination eradicated the disease saving an estimated 1.35 billion annually in vaccination + treatment costs. Hygiene + vaccines are the highest-ROI public-health investment in human history.
Q 7.43
``Prevention is better than cure''. Comment.
Concept used. The aphorism captures a public-health principle: stopping a disease from occurring is more efficient (in cost, suffering, and outcomes) than treating it after onset. Many infectious and lifestyle diseases lack reliable cures, so prevention is the most powerful intervention.
Disease has direct and indirect costs (medication, hospitalisation, lost work, family stress). Prevention avoids all of these.
Many diseases have no cure (AIDS, polio, rabies once symptoms appear). Vaccination or hygiene prevents them outright.
Even curable diseases (typhoid, malaria) leave long-term complications. Prevention avoids those sequelae.
Preventive tools include vaccination, hygiene, clean water, balanced diet, exercise, vector control (mosquito nets, indoor spraying), and screening (Pap smear, mammography).
Prevention is cheaper, more effective and avoids suffering; especially crucial for incurable diseases (AIDS, polio, rabies) and for diseases with long-term sequelae.
SC
Sneha Chatterjee
M.Sc Biotechnology, AIIMS Delhi
Verified Expert
Strategic angle. Three pillars of argument: cost, incurability, complications.
Cost: vaccines are 10x to 100x cheaper than treating the disease they prevent.
Incurability: a cured disease still has cases that fail therapy; prevented cases have zero failures.
Sequelae: polio survivors face lifelong paralysis even after the infection clears.
Cross-check. Cross-check via NCERT 8.3. Lymphoid organs are dedicated to lymphocyte production, maturation or activation. Bone marrow + thymus (primary), spleen + lymph nodes + tonsils + Peyer's patches + appendix (secondary). Pancreas is a digestive (acini) + endocrine (islets) organ — never lymphoid.
Prevention saves cost, suffering and lives, especially for incurable or sequelae-causing diseases.
Q 7.44
Explain any three preventive measures to control microbial infections.
Concept used. Microbial infections can be controlled at three points: (i) at the source (pathogen reservoir), (ii) during transmission, and (iii) at the host (immunity). Public-health programmes target all three.
Personal and public hygiene. Wash hands before meals; keep food covered; dispose of garbage; provide clean drinking water; treat sewage. This interrupts faecal–oral transmission of typhoid, cholera, hepatitis A, and amoebiasis.
Vector control. Eliminate breeding sites of mosquitoes (stagnant water); use insecticides and bed nets; introduce larvivorous fish (Gambusia). This breaks transmission of malaria, dengue, chikungunya, filariasis.
Vaccination (immunisation). Routine vaccines (DPT, OPV, MMR, BCG, Hepatitis-B) prime the immune system so the host clears the pathogen before disease develops. This has eradicated smallpox and brought polio and measles to near-elimination.
Three preventive measures: (1) personal & public hygiene; (2) vector control; (3) vaccination.
PN
Priya Nair
M.Sc Microbiology, JNU
Verified Expert
Strategic angle. Memorise three pillars: hygiene, vector control, vaccination. One example for each.
Cross-check. Cross-check via thymic involution. The thymus peaks in childhood and shrinks dramatically after puberty — its lymphoid tissue is replaced by adipose. This explains weaker vaccine responses in the elderly. Pituitary, pineal and thyroid all remain roughly constant in adulthood.
Hygiene + vector control + vaccination.
HIV life-cycle drug targets. Each step has a drug class: entry (maraviroc), reverse transcription (zidovudine NRTI, nevirapine NNRTI), integration (raltegravir), translation/processing (lopinavir protease inhibitor), budding (no licensed drug yet). HAART combines ≥ 3 classes to suppress viral load below detection limits (<50 copies/mL).
Q 7.45
In the given flow diagram, the replication of retrovirus in a host is shown. Observe and answer the following questions.
(a) Fill in (1) and (2)
(b) Why is the virus called retrovirus?
(c) Can the infected cell survive while viruses are being replicated and released?
Concept used. A retrovirus (e.g. HIV) has an RNA genome and the enzyme reverse transcriptase, which copies the viral RNA into double-stranded cDNA (viral DNA) inside the host. The viral DNA integrates into the host chromosome as a provirus. The integrated provirus is later transcribed and translated by the host machinery to produce new viral RNA and proteins, which assemble into new virions that bud out of the host cell.
Fig. 8.2 (NCERT Exemplar Class 12 Biology Chapter 8): flow of retrovirus replication.
(a) Fill in the blanks.
(1) Viral DNA formed by reverse transcription of viral RNA.
(2) New viral RNA (and viral proteins) produced from the integrated provirus.
(b) The virus is called retrovirus because it reverses the normal direction of genetic information flow. The Central Dogma says DNA → RNA → protein; retroviruses run the first arrow backwards: RNA → DNA, using reverse transcriptase.
(c) The infected cell ultimately dies. While viruses are being produced, the cell's resources are consumed, its membrane is breached as new virions bud out, and (for HIV) the host CD4 T-cell is destroyed within days to weeks. Some retroviruses can persist in a latent state, but eventually production of virions kills the host cell.
(1) Viral DNA; (2) new viral RNA and proteins. ``Retro'' = reverse: RNA → DNA via reverse transcriptase. The host cell typically dies as virions are released.
AI
Aarav Iyer
Ph.D Molecular Biology, NCBS Bangalore
Verified Expert
Picture-first. Read the flow chart: viral RNA → ? → integration → ? → new viruses. The two blanks are the intermediate products: viral DNA and new viral RNA.
Blank 1: between ``reverse transcription'' and ``viral DNA incorporates into host genome'' is the viral DNA itself.
Blank 2: between ``Viral DNA incorporates into host genome'' and ``Viruses come out of the host cell'' is the new viral RNA + proteins being made.
Name origin: ``retro'' because RNA → DNA reverses the Central Dogma's flow.
Host cell: cannot survive long; CD4 T-cells die.
Cross-check. Cross-check via malaria pathology. Plasmodium digests host haemoglobin, releasing toxic haem; the parasite polymerises it into inert haemozoin crystals. When RBCs synchronously rupture every 48–72 hours, haemozoin + merozoites spill into blood and trigger the chills-fever-sweat cycle.
1 = viral DNA; 2 = new viral RNA; retro because RNA → DNA via RT; host cell dies.
Q 7.46
``Maintenance of personal and public hygiene is necessary for prevention and control of many infectious diseases''. Justify the statement giving suitable examples.
Concept used. Many infectious diseases are transmitted by routes that hygiene directly interrupts: faecal–oral (contaminated food/water), respiratory droplet (coughs, sneezes), and contact (skin, fomites). Good hygiene practices block these routes.
Personal hygiene.
Hand-washing before meals and after toilet: prevents typhoid, cholera, amoebiasis, hepatitis A.
Bathing and clean clothes: prevent ringworm, scabies, lice.
Covering nose/mouth while coughing: prevents pneumonia, influenza, TB.
Public: clean water → cholera; vector control → malaria.
Cross-check. Cross-check via fungal taxonomy. Dermatophyte trio for ringworm: Microsporum (hair/skin), Trichophyton (skin/nails), Epidermophyton (skin). ``Macrosporum'' is a fabricated distractor playing on the Micro/Macro prefix swap.
Hygiene blocks faecal–oral, droplet, and vector-borne transmission of major infectious diseases.
Symptom recall. Ascariasis = intestinal worm; ringworm = scaly skin patches; typhoid = step-ladder fever + rose-spots + relative bradycardia; pneumonia = consolidation → dyspnea + chills; common cold = nasal discharge; filariasis = lymphatic obstruction → elephantiasis of leg or scrotum. NCERT's Table 8.1 is the source.
Q 7.47
The following table shows certain diseases, their causative organisms and symptoms. Fill the gaps.
(i) Ascariasis – Ascaris – ?
(ii) ? – Trichophyton – dry, scaly skin lesions
(iii) Typhoid – ? – high fever, weakness, headache, stomach pain, constipation
(iv) Pneumonia – Streptococcus pneumoniae – ?
(v) ? – Rhinoviruses – nasal congestion, sore throat, cough, headache
(vi) Filariasis – ? – inflammation in lower limbs
Concept used. Each NCERT-listed infectious disease has a fixed (causative organism, key symptom) tuple. The table tests recall of these tuples.
Fill each gap.
(i) Ascaris (round worm) causes internal bleeding, muscular pain, fever, anaemia and blockage of intestinal passage.
(ii) Trichophyton causes ringworm.
(iii) Typhoid is caused by Salmonella typhi (a bacterium).
(iv) Pneumonia symptoms: fever, chills, cough, difficulty in breathing, headache; lips and finger-tips may turn grey/blue in severe cases.
(v) Rhinoviruses cause the common cold.
(vi) Filariasis is caused by Wuchereria (W. bancrofti and W. malayi).
(i) intestinal blockage, anaemia, pain; (ii) Ringworm; (iii) Salmonella typhi; (iv) fever, chills, cough, dyspnea; (v) Common cold; (vi) Wuchereria.
AB
Ananya Bhat
M.Sc Microbiology, JNU
Verified Expert
Strategic angle. Mass recall question; pair each fragment to its NCERT entry.
Pair ``Trichophyton'' with ringworm.
Pair ``typhoid'' with Salmonella typhi.
Pair ``Rhinovirus'' with common cold.
Pair ``filariasis'' with Wuchereria.
Cross-check. Cross-check via heterozygote advantage. Carriers (HbAHbS) have RBCs that sickle when invaded by Plasmodium falciparum and are cleared too quickly by the spleen for the parasite to complete schizogony. The allele's geographic frequency in Africa/India tracks the malaria belt — Darwinian selection at work.
See main solution.
Q 7.48
The outline structure of a drug is given below.
(a) Which group of drugs does this represent?
(b) What are the modes of consumption of these drugs?
(c) Name the organ of the body which is affected by consumption of these drugs.
Concept used. The structure shown is that of a cannabinoid (the THC / cannabinol skeleton — a phenolic compound with a long alkyl side chain). Cannabinoids are derived from the inflorescences of Cannabis sativa.
Fig. 8.3 (NCERT Exemplar Class 12 Biology Chapter 8): outline structure of a cannabinoid (THC family).
(a) The compound represents the cannabinoids group (marijuana, hashish / charas, ganja).
(b) Cannabinoids are usually consumed by inhalation (smoking) of dried inflorescences or hashish, and by oral ingestion (in food preparations such as bhang).
(c) The principal organs affected are the cardiovascular system (raised heart rate, blood pressure) and the central nervous system / brain (impaired memory, distorted perception, hallucinations).
(a) Cannabinoids; (b) inhalation (smoking) or oral ingestion; (c) cardiovascular system and brain (CNS).
YK
Yash Kumar
M.Sc Biotechnology, AIIMS Delhi
Verified Expert
Picture-first. The structure has the tell-tale features of cannabinoids: a phenolic aromatic ring fused to a pyran or cyclohexene, with a long alkyl side chain.
Aromatic ring + OH groups + long alkyl chain → cannabinoid skeleton.
Sources: Cannabis sativa.
Modes: smoking, ingestion.
Targets: brain (CNS) and heart.
Cross-check. Cross-check via receptor biology. HIV gp120 binds CD4 + co-receptor (CCR5/CXCR4) — only T-helper cells, macrophages and dendritic cells display this combination. Plasmodium merozoites bind glycophorin on RBCs. S. typhi invades intestinal M-cells. Same logic, different receptor-tissue pair each time.
Cannabinoids; smoking/ingestion; brain + heart.
Q 7.49
Give the full form of CT and MRI. How are they different from each other? Where are they used?
Concept used.CT (Computed Tomography) uses multiple X-ray projections combined by computer reconstruction to produce cross-sectional images of the body. MRI (Magnetic Resonance Imaging) uses a strong magnetic field and radio-frequency pulses to align hydrogen nuclei in the body and detect their relaxation signals, producing soft-tissue images. Both are non-invasive imaging modalities used in cancer detection.
Full forms:
CT = Computed Tomography
MRI = Magnetic Resonance Imaging
Differences.
CT uses ionising X-rays; MRI uses non-ionising magnetic field + radio waves.
CT is faster (seconds), MRI is slower (15–45 minutes).
CT excels for bone and acute haemorrhage; MRI excels for soft tissues (brain, spinal cord, ligaments, tumours).
CT has some radiation exposure; MRI has no ionising radiation.
Uses: both detect tumours and structural abnormalities of internal organs; CT is commonly used for emergency head/chest imaging and cancer staging; MRI for brain, spine, soft-tissue tumours and joints.
CT = Computed Tomography (X-rays); MRI = Magnetic Resonance Imaging (magnetic field + radio waves). CT is fast and good for bone/haemorrhage; MRI is non-ionising and good for soft tissue. Both detect cancers and structural lesions.
KJ
Krishna Joshi
Ph.D Molecular Biology, NCBS Bangalore
Verified Expert
Strategic angle. Three-row table: full form, physical principle, best use case.
MRI: magnetic resonance of 1H; brain, soft tissue, tumours.
Both used in cancer detection and staging.
Cross-check. Cross-check via ELISA biology. The test detects host antibodies against HIV envelope/core proteins. Two ELISA positives + Western blot confirmation = HIV-positive. Immune-suppression points specifically to AIDS phase (CD4 count <200 cells/μL), not asymptomatic carriage.
CT = X-ray tomography (bone/trauma); MRI = magnetic resonance (soft tissue/brain). Both image internal pathology including tumours.
Therapeutic-vs-recreational dose. Morphine clinical dose = 5–10 mg IM for severe pain; recreational heroin = 50–200 mg with rapid IV onset (high abuse liability). Therapeutic cocaine = 4% topical for ENT mucosal anaesthesia; recreational = snorted or smoked at 10–100× doses. Dose makes the medicine — and the poison.
Q 7.50
Many secondary metabolites of plants have medicinal properties. It is their misuse that creates problems. Justify the statement with an example.
Concept used. Plants produce many secondary metabolites (alkaloids, terpenes, phenolics) that have powerful pharmacological action. Many become medicines when used in the right dose for the right indication, and become drugs of abuse when misused.
Example: opioids from Papaver somniferum.
Morphine, extracted from opium poppy latex, is one of the most effective analgesics (pain killers) used in surgery, cancer pain, and palliative care.
The same compound, when used recreationally and at higher doses (as heroin / smack), causes addiction, respiratory depression and death.
Other examples: cocaine (medical anaesthetic vs. stimulant abuse); cannabinoids (chronic pain relief vs. recreational marijuana); barbiturates (anti-seizure vs. abuse).
Conclusion: secondary metabolites are double-edged; medical control of dose and indication separates therapy from abuse.
Plant secondary metabolites (e.g. morphine from opium poppy) are valuable medicines (analgesics) but become addictive drugs (heroin) when misused. Dose and indication control matter.
DK
Diya Kapoor
M.Sc Biotechnology, AIIMS Delhi
Verified Expert
Quick reading. The same molecule can be a medicine or a drug of abuse; dose + context define which.
Cross-check. Cross-check via haematopoiesis. All lymphocytes originate from a haematopoietic stem cell in bone marrow. B-cells stay and complete maturation locally. T-precursors migrate to the thymus, where positive + negative selection eliminates self-reactive clones; mature T-cells then seed secondary lymphoid organs.
Same molecule, medicine or abuse — depends on dose and indication.
Phytochemical context. Secondary metabolites give plants flavour (peppermint terpenes), colour (anthocyanins), defence (nicotine, caffeine repel insects), UV protection (flavonoids), and antibiotic action (penicillin, taxol). Humans exploit them as drugs (quinine for malaria, morphine for pain, vincristine for leukaemia, paclitaxel for breast cancer).
Q 7.51
Why cannabinoids are banned in sports and games?
Concept used. Cannabinoids (marijuana, charas, hashish) are banned by sports regulatory bodies (WADA, IOC) because they impair athletic performance, alter judgement, and are addictive.
Cannabinoids affect the central nervous system: they alter perception, slow reaction time, impair coordination and short-term memory.
They affect the cardiovascular system: increase heart rate and blood pressure.
They can be used to mask pain and fatigue, giving an unfair edge in endurance events.
Athletes risk addiction and long-term cognitive and respiratory damage.
Hence cannabinoids are on the WADA prohibited list for in-competition use.
Cannabinoids impair CNS function, raise cardiovascular load, mask pain/fatigue, and are addictive — hence banned by sporting bodies.
RB
Rohit Banerjee
M.Sc Microbiology, JNU
Verified Expert
Strategic angle. Two reasons sport bodies ban a substance: performance enhancement and health risk. Cannabinoids tick both.
Performance: alters mood, can mask pain, blunts response.
Health: addictive, cardiotoxic.
Cross-check. Cross-check via cause–disease table. Microsporum causes ringworm (a fungal skin disease), while filariasis is caused by helminths Wuchereria bancrofti/W. malayi, transmitted by Culex. The other three pairs (rhinovirus–cold, Salmonella–typhoid, Plasmodium–malaria) are NCERT-correct.
Banned due to performance distortion and health hazard.
Q 7.52
What is secondary metabolism?
Concept used.Primary metabolism is the universal set of biochemical pathways needed for growth and survival (glycolysis, TCA cycle, protein synthesis). Secondary metabolism produces compounds (alkaloids, terpenes, phenolics, flavonoids) that are not strictly required for growth but provide ecological functions such as defence against herbivores, antimicrobial activity, attraction of pollinators, or UV protection.
Define secondary metabolites: organic compounds produced by plants (and microbes) that are not directly involved in basal growth or reproduction.
Note their importance: many are starting points for medicines and drugs.
Secondary metabolism produces compounds (alkaloids, terpenoids, phenolics) not essential for plant growth but useful for defence and ecological interactions; many are valuable medicines.
PV
Priya Verma
Ph.D Molecular Biology, NCBS Bangalore
Verified Expert
Quick reading. Primary = essential for life. Secondary = ecological/defensive.
Primary: glycolysis, photosynthesis, AA synthesis.
Secondary: morphine, nicotine, terpenes.
Cross-check. Cross-check via T-cell function. The thymus is the only site of T-cell maturation. Without it: no cytotoxic T-cells → intracellular pathogens (TB, viruses) cannot be cleared; no helper T-cells → B-cells receive no co-stimulation → antibody titres collapse. DiGeorge syndrome is the clinical parallel.
Secondary metabolism = non-essential biosynthesis of defensive/ecological molecules.
Q 7.53
Drugs and alcohol give short-term `high' and long-term `damages'. Discuss.
Concept used. Most psychoactive drugs and alcohol act on the brain's reward pathway (dopamine release in the nucleus accumbens). This produces a short-term euphoria. With repeated use, the brain adapts (tolerance, dependence), and chronic use damages multiple organ systems.
Damage phase: tolerance, dependence, organ damage, withdrawal.
Cross-check. Cross-check via gut defence stack. Mouth (lysozyme), stomach (HCl pH 1.5–2 kills most bacteria), small intestine (mucus + commensal flora + Peyer's patches IgA). All are present from birth, non-specific, and do not improve with repeated exposure — hallmarks of innate immunity.
Drugs/alcohol exchange minutes of high for years of damage to brain, liver, heart, kidneys, society.
Q 7.54
Diseases like dysentery, cholera, typhoid etc., are more common in over crowded human settlements. Why?
Concept used. These are all faecal–oral transmitted diseases caused by ingestion of food or water contaminated with faecal pathogens. Overcrowding magnifies every link in their transmission chain.
Inadequate sanitation in crowded slums leads to open defecation or leaking sewers, contaminating water sources.
Limited clean water means people share water sources; one contamination event infects many.
Crowding accelerates person-to-person transmission via hand contact and shared utensils.
Flies multiply on uncollected garbage and mechanically transfer pathogens to food.
Poor nutrition and stress in crowded settings reduce host resistance.
Combined, all these factors keep the basic reproductive number R0 above 1, sustaining the disease.
Overcrowding + poor sanitation + shared water + flies + low nutrition all amplify faecal–oral transmission of dysentery, cholera, typhoid.
IS
Ishita Singh
M.Sc Microbiology, JNU
Verified Expert
Strategic angle. Identify the four transmission factors that crowding worsens: sanitation, water, contact, flies.
Sanitation breaks → faeces → water.
Water shared → pathogen multiplied across people.
Crowd contact → direct spread.
Flies + garbage → food contamination.
Cross-check. Cross-check via infant nutrition. Colostrum's protein-rich, vitamin-A-rich, IgA-rich profile is uniquely matched to neonatal needs; lactoferrin sequesters iron from gut microbes; oligosaccharides feed Bifidobacterium; passive antibody coverage spans roughly the first 4–6 months while the infant's own immune system matures.
Crowding amplifies sanitation, water and contact-based transmission of faecal pathogens.
Q 7.55
From which plant cannabinoids are obtained? Name any two cannabinoids. Which part of the body is affected by consuming these substances?
Concept used. Cannabinoids are a class of psychoactive compounds extracted from the inflorescences and resin of Cannabis sativa (Indian hemp).
Source plant: Cannabis sativa.
Two cannabinoids (common preparations): marijuana (from leaves/inflorescences), hashish or charas (from resin), ganja (from female flowering tops), bhang (from leaves, ingested orally). Two examples: marijuana and hashish (charas). The principal active molecule is Δ9-tetrahydrocannabinol (THC).
Body parts affected: the central nervous system (brain) — distortion of perception, impaired memory, hallucinations — and the cardiovascular system — raised heart rate, blood pressure.
Cross-check. Cross-check via IgE-mast cell axis. Urban triggers (PM2.5, NOx, dust mites, pet dander, mould, pollen) sensitise B-cells → IgE binds mast cells → allergen cross-links IgE → mast cell degranulates → histamine release → sneezing, congestion, wheeze, urticaria, anaphylaxis. Hygiene-hypothesis ties it to childhood microbial deprivation.
Q 7.56
In the metropolitan cities of India, many children are suffering from allergy/asthma. What are the main causes of this problem. Give some symptoms of allergic reactions.
Concept used.Allergy is a hypersensitive response of the immune system to harmless environmental antigens called allergens (dust, pollen, mould, animal dander, pollutants, certain foods, drugs). The response is mediated by IgE antibodies, which bind to mast cells, triggering release of histamine and other mediators.
Main causes in metropolitan settings.
Air pollution: PM2.5 and PM10 particulates, NOx, SO2, smoke.
Indoor allergens: house-dust mites, pet dander, mould.
Pollen from urban trees / weeds.
Reduced microbial exposure in childhood (hygiene hypothesis): the immune system, lacking microbial training, over-reacts to harmless antigens.
Tobacco smoke (active and passive).
Symptoms of allergic reactions.
Sneezing, runny nose, nasal congestion.
Watery, itchy eyes.
Difficulty breathing, wheezing, cough (asthma).
Skin rashes, hives, itching.
In severe cases, anaphylaxis (drop in blood pressure, swelling of airway, shock).
Antihistamines and steroids are used for symptom relief; avoidance of triggers is the long-term management.
Causes: urban air pollution, dust mites, pet dander, pollen, low microbial exposure. Symptoms: sneezing, watery eyes, wheezing, rash, breathing difficulty.
TK
Tara Kapoor
M.Sc Biotechnology, AIIMS Delhi
Verified Expert
Strategic angle. The question has two parts: causes (environment) and symptoms (clinical signs).
Cross-check. Cross-check via paracrine antiviral signalling. Infected cell senses double-stranded viral RNA via PRRs → secretes IFN → IFN binds receptors on neighbour cells → JAK/STAT cascade → antiviral state. By the time the virus arrives at the neighbour, its replication machinery is pre-blocked.
Vaccine taxonomy. Live attenuated (OPV, MMR, BCG, Yellow Fever) — strong, long-lasting immunity, mucosal coverage; contraindicated in immunosuppressed. Killed/inactivated (Salk IPV, Hep A, rabies, flu shot) — safer but needs boosters. Subunit/recombinant (Hep B, HPV) — extra-safe, scalable. Toxoid (DT, TT) — for toxin-mediated diseases. mRNA (COVID) — newest platform.
Q 7.57
What is the basic principle of vaccination? How do vaccines prevent microbial infections? Name the organism from which hepatitis B Vaccine is produced.
Concept used.Vaccination is the deliberate introduction of an antigen (in a safe form) into the body so that the immune system generates a specific response and memory cells without causing disease. The principle exploits immunological memory.
Principle. Expose the immune system to a weakened (attenuated), killed, or sub-unit form of a pathogen. The system mounts a primary response, produces antibodies, and most importantly generates memory B and T-cells.
Mechanism of protection. On future natural infection, memory cells recognise the antigen and trigger a fast, large secondary response that clears the pathogen before disease develops.
Hepatitis B vaccine source. The recombinant Hepatitis B vaccine is produced by inserting the gene for HBsAg (Hepatitis B surface antigen) into yeast (Saccharomyces cerevisiae). The yeast cell expresses the surface antigen, which is purified and used as the vaccine.
Vaccination principle: prime the immune system with a safe antigen to generate memory cells. Mechanism: rapid secondary response on real infection. Hep-B vaccine: recombinant HBsAg from yeast Saccharomyces cerevisiae.
DN
Diya Nair
Ph.D Molecular Biology, NCBS Bangalore
Verified Expert
Strategic angle. Three parts: principle, mechanism, Hep-B source. Cover each in one or two lines.
Principle: induce memory without disease.
Mechanism: secondary response on infection clears pathogen pre-symptomatically.
Cross-check. Cross-check via hallmarks of cancer. Normal cell: contact-inhibited, finite divisions, apoptosis on damage. Cancer cell: lost contact inhibition, telomerase reactivated (immortal), apoptosis-resistant, self-sufficient growth signals, invasive, metastatic. Transformation needs 4–7 driver mutations activating oncogenes / silencing tumour suppressors.
Six hallmarks of cancer (Hanahan & Weinberg classic): (1) self-sufficient growth signals, (2) insensitive to anti-growth signals, (3) evading apoptosis, (4) limitless replicative potential (telomerase), (5) sustained angiogenesis, (6) tissue invasion + metastasis. NEET expects (1) loss of contact inhibition, (2) immortality, (3) metastatic ability as the headline differences.
Q 7.58
What is cancer? How is a cancer cell different from the normal cell? How do normal cells attain cancerous nature?
Concept used.Cancer is a disease characterised by uncontrolled cell division and the ability to invade and spread (metastasise). Normal cells exhibit contact inhibition (stop dividing on contact with neighbours) and obey growth-control checkpoints; cancer cells lose these.
Definition of cancer. Uncontrolled, invasive proliferation of cells that can spread (metastasise) to distant organs.
How cancer cells differ from normal cells.
Normal: contact inhibition; cancer: no contact inhibition.
Normal: differentiated, stays in tissue; cancer: poorly differentiated, invades surrounding tissue and metastasises.
Normal: dies on damage (apoptosis); cancer: resists apoptosis.
Normal: dependent on growth signals; cancer: self-sufficient in growth signals.
How normal cells become cancerous. Normal cells contain proto-oncogenes (which promote cell division) and tumour-suppressor genes (which restrain it). Mutations or activations (by chemical carcinogens like tobacco tar; physical carcinogens like UV/X-rays; biological carcinogens like HPV, HBV, EBV) convert proto-oncogenes into oncogenes and inactivate tumour-suppressor genes. Accumulation of multiple such mutations transforms a normal cell into a cancer cell.
Cancer = uncontrolled, invasive cell growth. Cancer cells lack contact inhibition and apoptosis. Normal cells become cancerous through carcinogen-induced mutations that activate oncogenes and inactivate tumour-suppressor genes.
AP
Aanya Patel
M.Sc Biotechnology, AIIMS Delhi
Verified Expert
Strategic angle. Three sub-questions: definition, normal-vs-cancer differences, transformation mechanism.
Cross-check. Cross-check via H2 L2 geometry. Two heavy + two light chains form a Y; the variable regions at the two Fab tips are the antigen-binding sites (A); the short outer polypeptide is the light chain (B); the long inner one running through the stem is the heavy chain (C). Inter-chain S–S bonds hold it together.
Cancer: uncontrolled invasive growth. Cancer cells lack contact inhibition + apoptosis. Caused by carcinogen-induced mutations.
Allergy management ladder. Step 1: identify and avoid the trigger via skin prick test. Step 2: oral antihistamine (cetirizine, loratadine) for mild symptoms. Step 3: nasal corticosteroid spray for chronic rhinitis. Step 4: leukotriene antagonist (montelukast) for asthma overlap. Step 5: allergen immunotherapy (sublingual or subcutaneous desensitisation). Step 6: emergency epinephrine auto-injector for anaphylaxis history.
Q 7.59
A person shows strong unusual hypersensitive reactions when exposed to certain substances present in the air. Identify the condition. Name the cells responsible for such reactions. What precaution should be taken to avoid such reactions.
Concept used. The described condition is allergy, an IgE-mediated immediate hypersensitivity. The cells most directly responsible are mast cells (and basophils), which carry IgE on their surface and release histamine on antigen binding.
Condition: allergic reaction (Type I hypersensitivity).
Cells responsible:
B-cells / plasma cells produce specific IgE.
IgE binds to mast cells and basophils via Fc receptors.
On re-exposure to allergen, mast cells degranulate and release histamine, leukotrienes and prostaglandins.
Precautions.
Identify and avoid the allergen (pollen, dust, dander, perfumes).
Use air filters / masks in polluted or pollen-heavy environments.
Keep house clean and dust-free.
Use prescribed antihistamines or steroidal inhalers; carry an EpiPen for severe allergies.
Condition: allergy. Cells: mast cells & basophils (loaded with IgE, releasing histamine). Precaution: avoid allergens, use masks/filters, take antihistamines.
RP
Riya Pillai
M.Sc Microbiology, JNU
Verified Expert
Strategic angle. Three parts: name → cells → precaution.
Name: allergy / hypersensitivity.
Cells: mast cells release histamine; B-cells produced the IgE.
Avoid trigger; medications for symptoms.
Cross-check. Cross-check via dependence neurobiology. Chronic drug exposure downregulates receptor density to compensate for excess agonism. Sudden absence leaves the brain ``hypo-stimulated'' → anxiety, tremors, autonomic surge (sweating, palpitations), GI upset, plus intense craving driven by dopamine-pathway adaptation.
Clinical anchor. The 1954 Boston twin-kidney transplant by Joseph Murray (later Nobel laureate) succeeded only because donor and recipient were identical twins — no rejection without any of today's immunosuppressants. The breakthrough validated the MHC theory of rejection and launched modern transplant medicine.
Q 7.60
For an organ transplant, it is an advantage to have an identical twin. Why?
Concept used.Graft rejection is driven by the recipient's T-cells recognising foreign MHC molecules on donor cells. Identical (monozygotic) twins share 100% of their DNA, including identical MHC alleles, so the donor's tissue is immunologically indistinguishable from the recipient's own.
In an unrelated donor, MHC differences trigger cytotoxic T-cell response → rejection.
Identical twins share the same MHC haplotypes → the recipient's T-cells see no foreign MHC.
The transplanted organ is recognised as ``self'' → no rejection.
The recipient does not need life-long immunosuppression and has the best outcome.
Identical twins share identical MHC; the transplanted organ is treated as self, so no immune rejection occurs.
KS
Krishna Sharma
Ph.D Molecular Biology, NCBS Bangalore
Verified Expert
Strategic angle. Genetic identity = MHC identity = no foreign antigens = no rejection.
Same genome ⇒ same MHC.
Same MHC ⇒ no T-cell mediated rejection.
Cross-check. Cross-check via aerosol physics. Cool, dry air dries the respiratory mucus and impairs ciliary clearance; AC systems re-circulate the same air; crowding concentrates respiratory droplets per cubic metre. One infectious person (rhinovirus, influenza, SARS-CoV-2) can transmit to many in a short time window.
Same MHC, no rejection.
Q 7.61
What are lifestyle diseases? How are they caused? Name any two such diseases.
Concept used.Lifestyle diseases are non-communicable diseases caused largely by the way people live — diet, physical activity, smoking, alcohol use, stress — rather than by infection.
Definition: chronic non-infectious diseases linked to modifiable lifestyle factors.
Causes:
Unhealthy diet (high fat, salt, sugar).
Lack of physical activity.
Tobacco smoking and alcohol consumption.
Chronic stress and poor sleep.
Obesity (often a consequence of the above).
Examples (any two):
Type 2 diabetes mellitus.
Hypertension and cardiovascular disease.
Obesity.
Certain cancers (lung, oral, colorectal).
Chronic obstructive pulmonary disease (COPD).
Lifestyle diseases are non-infectious chronic disorders driven by diet, inactivity, smoking, alcohol and stress. Examples: type 2 diabetes, hypertension/heart disease, obesity, certain cancers.
Cross-check. Cross-check via population genetics. Hardy-Weinberg with selection coefficients: HbAHbA dies of falciparum; HbSHbS dies of anaemia; heterozygotes survive both. Equilibrium allele frequency for HbS stabilises at ∼ 0.1 in malaria-endemic populations — a textbook case of balanced polymorphism.
Lifestyle diseases: chronic NCDs from modifiable habits; e.g. diabetes, hypertension.
Q 7.62
If there are two pathogenic viruses, one with DNA and other with RNA, which would mutate faster? And Why?
Concept used.Mutation rate depends on the fidelity of the polymerase that copies the viral genome. DNA polymerases generally have a 3'→5' exonuclease proof-reading activity, lowering the error rate to about 10-8 per base. Most viral RNA polymerases (and reverse transcriptase) lack proof-reading, so errors of about 10-4 per base are typical — roughly 10000 times more.
DNA virus: replicated by DNA polymerase with proof-reading → low error rate.
RNA virus: replicated by RNA-dependent RNA polymerase (or by reverse transcriptase for retroviruses) without proof-reading → high error rate.
Therefore the RNA virus mutates much faster.
Practical consequence: RNA viruses (influenza, HIV, SARS-CoV-2, hepatitis C) evolve rapidly, evade immunity, and need annual or strain-specific vaccines; DNA viruses (smallpox, herpes) are much more stable, so a single vaccine often suffices.
RNA virus mutates faster. RNA polymerase / reverse transcriptase lacks proof-reading, so error rate is 104 times higher than DNA polymerase.
AI
Aaditya Iyer
Ph.D Molecular Biology, NCBS Bangalore
Verified Expert
Strategic angle. Compare polymerase fidelity. RNA polymerases lack proof-reading; DNA polymerases have it.
Mutation rate ∼ inversely proportional to proof-reading.
RNA virus has no proof-reading ⇒10-4 errors/base.
DNA virus has proof-reading ⇒10-8 errors/base.
Cross-check. Cross-check via lymph-node architecture. Cortex (B-cell follicles, germinal centres for affinity maturation) + paracortex (T-cell zone) + medulla (plasma cells). Antigens enter via afferent lymphatics; activated lymphocytes leave via efferent lymphatics into thoracic duct → blood circulation.
RNA viruses mutate 104 times faster than DNA viruses because their polymerases lack proof-reading.
Time-keeping anchor.P. vivax and P. ovale: fever every 48 h (tertian); P. malariae: every 72 h (quartan); P. falciparum: 36–48 h, often irregular and the deadliest. Liver schizogony takes 1–2 weeks (the incubation period); RBC cycles take 48–72 h once symptoms begin.
Long Answer Type Questions (LA)
Q 7.63
Represent schematically the life cycle of a malarial parasite.
Concept used. The malarial parasite (Plasmodium spp., principally P. falciparum and P. vivax) is digenetic: it requires both a human host and a female Anopheles mosquito to complete its life cycle. Key stages: sporozoites (infective stage in mosquito saliva), schizonts and merozoites (asexual stages in liver and RBCs), and gametocytes (sexual stage taken up by mosquito).
Step 1 — Bite & sporozoite injection. A female Anopheles bites a human; sporozoites in her saliva enter the blood.
Step 2 — Liver schizogony. Sporozoites travel to the liver and infect hepatocytes; they multiply asexually (schizogony) into thousands of merozoites.
Step 3 — RBC schizogony. Liver merozoites burst out and invade RBCs. Inside RBCs they multiply again; the synchronous rupture of RBCs releases merozoites + haemozoin every 48–72 hours, causing the recurrent chills and high fever.
Step 4 — Gametocyte formation. Some merozoites differentiate into male and female gametocytes, the sexual stage.
Step 5 — Uptake by mosquito. When another mosquito bites the infected human, it ingests gametocytes with the blood meal.
Step 6 — Fertilisation in mosquito gut. Male and female gametes fuse to form a zygote (ookinete) in the mosquito gut; this becomes an oocyst on the gut wall.
Step 7 — Sporozoite formation. Each oocyst releases thousands of sporozoites that migrate to the mosquito's salivary glands, ready to infect the next person bitten.
!%
[See diagram in the PDF version]
Plasmodium life cycle: sporozoites (mosquito saliva) → liver schizogony → RBC schizogony (fever) → gametocytes → mosquito bite → zygote in gut → oocyst → sporozoites. A two-host cycle.
VB
Vivaan Banerjee
M.Sc Biotechnology, AIIMS Delhi
Verified Expert
Strategic angle. Memorise the cycle as a loop with two halves: human half (liver → RBC → gametocyte) and mosquito half (gut fertilisation → oocyst → salivary sporozoites).
Sporozoites enter human via bite.
Multiply in liver (exo-erythrocytic schizogony).
Burst out, infect RBCs (erythrocytic schizogony).
Form gametocytes; mosquito ingests them.
Zygote in gut → oocyst → sporozoites → salivary glands.
Cycle restarts on next bite.
Cross-check. Cross-check via memory-cell biology. First exposure: naive B/T cells take 1–2 weeks to expand and class-switch. Memory cells store the antigen-specific clone for years/decades. Second exposure: clonal burst in 2–3 days, IgG dominant, titres often 10–100× higher than primary.
Burden anchor. India is currently in the dual-burden phase: NCDs cause ∼ 65% of urban deaths (ICMR 2024 estimates), while infectious diseases still cause ∼ 30% of rural mortality. Health-system planning must address both — vaccine + sanitation coverage for rural, while expanding cardiology, oncology and mental-health services for urban populations.
Q 7.64
Compare the life style of people living in the urban areas with those of rural areas and briefly describe how the life style affects their health.
Concept used. Lifestyle determines exposure to risk factors and access to health resources. Urban and rural lifestyles differ in diet, physical activity, sanitation, pollution and stress, leading to characteristic disease patterns.
Urban lifestyle.
Sedentary work (desk jobs); little walking; reliance on motorised transport.
Diet rich in processed food, sugar, salt, fats.
High exposure to air pollution, noise pollution, light at night.
Higher levels of psychological stress, irregular hours.
Easy access to tobacco, alcohol.
Better access to hospitals and diagnostics.
Rural lifestyle.
Physical labour (farming, walking long distances).
Diet centred on cereals, vegetables, dairy; lower processed food.
Cleaner air but sometimes biomass cooking smoke indoors.
Poorer sanitation, drinking water, sewage in many areas.
Less access to vaccines, doctors, specialist care.
Health impacts.
Urban populations: high rates of diabetes, hypertension, obesity, heart disease, lung diseases (pollution, smoking), depression, anxiety, certain cancers.
Rural populations: high rates of infectious diseases (diarrhoea, typhoid, malaria, TB), malnutrition, anaemia, maternal and child mortality.
Conclusion. Urban lifestyle promotes non-communicable lifestyle diseases; rural lifestyle is dominated by communicable diseases and malnutrition. Both need different public-health responses.
Urban: sedentary, processed food, polluted air, stress → diabetes, hypertension, cancer. Rural: physical work, simpler diet, but poor sanitation → infections, malnutrition. Different lifestyles, different disease loads.
SV
Sneha Verma
M.Sc Microbiology, JNU
Verified Expert
Strategic angle. Compare four axes: physical activity, diet, environmental exposure, stress. Then map each to disease pattern.
Activity: rural high, urban low.
Diet: rural simpler, urban processed.
Environment: urban polluted; rural cleaner air but poor sanitation.
Stress: urban high.
Disease load: urban → NCDs; rural → infections.
Cross-check. Cross-check via retroviral life cycle. ART targets every viral step: NRTIs/NNRTIs block reverse transcriptase, integrase inhibitors stop provirus formation, protease inhibitors block virion maturation, fusion/entry inhibitors block CD4 binding. The disease (AIDS) is the late immunosuppressive phase of HIV infection.
Warning sign checklist. Sudden drop in grades, unexplained money requests, secretive phone behaviour, new friend circles, mood swings, weight/sleep changes, glassy eyes, neglected appearance, withdrawal from family hobbies. Any cluster of these in an adolescent warrants gentle but prompt parental conversation, school counsellor referral, and (if persistent) medical evaluation — early intervention multiplies recovery odds.
Q 7.65
Why do some adolescents start taking drugs? How can this be avoided?
Concept used. Adolescence is a phase of curiosity, identity formation, and peer influence; combined with stress and easy availability of drugs, it is a high-risk window for substance initiation.
Reasons adolescents start drugs.
Curiosity, thrill-seeking.
Peer pressure and the urge to be ``accepted''.
Stress: academic pressure, family problems, breakup.
Imitation of media (films, glamorised drug use).
Easy availability and lack of awareness about long-term harm.
Family history of substance use; modelling by parents/siblings.
Underlying depression, anxiety, low self-esteem.
Prevention strategies.
Parental support: open communication, monitoring without coercion.
Education: school programmes on the science of addiction, real-life consequences.
Peer mentoring: connecting at-risk teens with positive role models.
Mental-health support: counselling, treatment of underlying depression/anxiety.
Legal enforcement: limit access of drugs to minors.
Seek professional help early at first signs (mood change, isolation, falling grades, money problems).
Key message. Prevention is most effective in early adolescence, before the first use. Once dependence sets in, recovery is harder.
Curiosity, peer pressure, stress, family environment and easy availability drive adolescent drug initiation. Prevention: parental support + education + mental-health care + recreation + early intervention.
KP
Karan Pillai
Ph.D Molecular Biology, NCBS Bangalore
Verified Expert
Strategic angle. Two-column: cause → counter-measure. Tackle each cause with a specific prevention.
Cause peer pressure → assertiveness training.
Cause stress → counselling, sports.
Cause curiosity → honest education on consequences.
Cause availability → legal enforcement.
Cross-check. Cross-check via active vs passive. Active = host's own antibodies + memory cells; slow onset (1–2 weeks), long-lasting. Passive = preformed antibodies given; immediate but lasts only weeks. Vaccines drive active; colostrum, antivenom and anti-tetanus globulin drive passive immunity.
Cause-by-cause prevention: peer pressure, stress, curiosity, availability all need targeted action plus parental support.
Withdrawal warning. Alcohol withdrawal can be fatal (unlike most drug withdrawals): delirium tremens carries ∼ 5% mortality from seizures and autonomic storm. Safe detox needs medical supervision with tapered benzodiazepines (diazepam, chlordiazepoxide), thiamine to prevent Wernicke encephalopathy, and IV fluids. Cold-turkey alcohol withdrawal at home in a heavy drinker is dangerous.
Q 7.66
In your locality, if a person is addicted to alcohol, what kind of behavioural changes do you observe in that person? Suggest measures to over come the problem.
Concept used. Chronic alcohol dependence produces predictable behavioural, social and physical changes. Recovery requires medical detoxification combined with long-term psychosocial support.
Aggression and domestic violence; financial problems.
Sleep disturbances; anxiety; depression.
Measures to overcome.
Recognise and admit the problem (the hardest step).
Seek professional medical help; supervised detoxification to manage withdrawal.
Counselling: individual therapy (CBT) and family counselling.
Support groups: Alcoholics Anonymous (AA) and peer-led groups.
Pharmacotherapy: disulfiram, naltrexone, acamprosate where indicated.
Removing access to alcohol; avoiding triggers and bars.
Replacement of social network with sober contacts.
Engagement in productive activity: work, hobbies, sports.
Family support, patience and absence of stigma.
Long-term follow-up to prevent relapse.
Behavioural changes: irritability, isolation, neglect, lying, domestic violence, tremors. Measures: medical detox + counselling + support groups + family support + relapse prevention.
DS
Diya Sharma
M.Sc Biotechnology, AIIMS Delhi
Verified Expert
Strategic angle. Split into observable changes + recovery roadmap.
Cross-check. Cross-check via NCERT 8.4 table. Benign tumour: encapsulated, slow, non-invasive, no metastasis, rarely fatal — surgical excision usually curative. Malignant tumour: no capsule, infiltrates, metastasises via blood/lymph, often fatal — needs combined surgery + radiotherapy + chemotherapy + sometimes immunotherapy.
Identify behavioural change patterns; recovery is multi-pronged: medical + psychological + social.
Modality matching. Localised tumour, accessible = surgery ± adjuvant radio (breast, colon). Localised but deep/inoperable = radio (cervix, head-neck). Systemic / blood (leukaemia, lymphoma) = chemotherapy. HER2+ breast / B-cell lymphoma = monoclonal antibodies (trastuzumab, rituximab). Melanoma, lung NSCLC = checkpoint inhibitors. Hormone-sensitive (breast ER+, prostate) = anti-hormones. Best results come from multi-modal combinations tailored to tumour stage and molecular profile.
Q 7.67
What are the methods of cancer detection? Describe the common approaches for treatment of cancer.
Concept used. Cancer treatment depends on early detection. Detection uses imaging, biopsy and molecular markers; treatment combines surgery, radiation, chemotherapy and immunotherapy.
Methods of cancer detection.
Biopsy and histopathological studies: take a small tissue sample, fix it, stain it, and examine under microscope; the gold standard.
Imaging: CT (X-ray cross-sections) and MRI (magnetic resonance) reveal tumour location and size; ultrasound and PET-CT are also used.
Molecular techniques: detection of oncogenic mutations and chromosomal translocations.
Mammography, Pap smear, colonoscopy for screening of common cancers.
Common approaches to treatment.
Surgery: removal of the primary tumour and adjacent lymph nodes; effective when the tumour is localised and accessible.
Radiotherapy: localised killing of cancer cells using ionising radiation (gamma rays, X-rays); often combined with surgery.
Chemotherapy: drugs that kill rapidly dividing cells (alkylating agents, antimetabolites, mitotic inhibitors). Used for systemic disease and metastases. Side effects include hair loss, anaemia, immunosuppression.
Immunotherapy: interferon-α (boosts the immune response against tumours), monoclonal antibodies (rituximab, trastuzumab), and modern checkpoint inhibitors.
Hormonal therapy: for hormone-sensitive cancers (tamoxifen for breast cancer).
Combination therapy: surgery + chemo + radio + immunotherapy together for the best outcomes.
Strategic angle. Diagnose → stage → treat. Each step has its own toolkit.
Detect: biopsy + imaging + markers.
Stage: how big, where spread.
Treat: surgery for local, radio for localised, chemo for systemic, immuno to boost host response.
Cross-check. Cross-check via combustion chemistry. The cigarette's lit tip burns at ∼ 600∘C, producing more incomplete-combustion products (benzo[a]pyrene, formaldehyde, nitrosamines, CO) than the smoker's filtered ∼ 900∘C puff. Passive smokers inhale these unfiltered, magnifying carcinogen dose per breath.
Detection: biopsy + CT/MRI + tumour markers. Treatment: surgery + radio + chemo + immunotherapy.
Treatment context. LSD has limited therapeutic role (under research for PTSD). Barbiturates have largely been replaced by safer benzodiazepines for anxiety/insomnia; they remain useful in anaesthesia (thiopental) and refractory seizures (phenobarbital). Amphetamines (methylphenidate, dextroamphetamine) are still prescribed for ADHD and narcolepsy at controlled low doses. The therapeutic-recreational gap is dose + supervision.
Q 7.68
Drugs like LSD, barbiturates, amphetamines, etc., are used as medicines to help patients with mental illness. However, excessive doses and abusive usage are harmful. Enumerate the major adverse effects of such drugs in humans.
Concept used.LSD (Lysergic Acid Diethylamide) is a hallucinogen. Barbiturates are CNS depressants used as sedatives. Amphetamines are CNS stimulants used in attention disorders. Abuse leads to dependence and serious organ damage.
LSD adverse effects.
Hallucinations, distortion of perception (lights, colours, sounds).
Paranoia, anxiety, panic attacks.
Bad ``trips'' can lead to suicide or violent accidents.
Flashbacks even weeks after use (HPPD).
Persistent psychotic disorders.
Barbiturate adverse effects.
Excessive sedation, drowsiness, slurred speech.
Respiratory depression — can be fatal at overdose.
Dependence and severe withdrawal (seizures).
Combination with alcohol multiplies the risk of death.
Cross-check. Cross-check via cost-benefit. Vaccines cost rupees per dose; treating the resulting disease costs lakhs (cancer chemotherapy, dialysis for diabetes complications). Add lost productivity and family suffering, and prevention saves an order-of-magnitude more value than cure — especially for incurable AIDS, polio, rabies.
Class-specific harms (hallucinations / sedation / hyperstimulation) plus universal harms (addiction, organ damage, overdose).
Programme metrics. National Pulse Polio Immunisation reached >170 million children per round at peak. India's last wild poliovirus case was 13 January 2011 (Howrah, West Bengal); WHO declared India polio-free on 27 March 2014. Switch to bivalent OPV (bOPV) + introduction of inactivated polio vaccine (IPV) in routine schedule guards against vaccine-derived poliovirus risk.
Q 7.69
What is Pulse Polio Programme of Government of India? What is OPV? Why is it that India is yet to eradicate Polio?
Concept used.Pulse Polio Immunisation (PPI) is a mass vaccination campaign launched in India in 1995, aimed at eradicating poliomyelitis. The slogan ``Do Boond Zindagi Ki'' (``Two drops of life'') refers to the drops of Oral Polio Vaccine (OPV) given to every child under 5 on National Immunisation Days.
Pulse Polio Programme. A nationwide campaign of giving polio drops to every child under 5, on selected dates each year, in addition to the routine vaccination schedule. The objective is to interrupt person-to-person transmission by saturating the population with immunity.
OPV (Oral Polio Vaccine). Developed by Albert Sabin. It is a live attenuated vaccine containing weakened polio virus, given orally as two drops. Advantages:
Easy to administer (no needles).
Induces both serum (IgG) and mucosal (IgA) immunity.
The attenuated virus is shed in stools and can passively immunise close contacts (herd effect).
Why eradication has been slow.
India was declared polio-free in 2014 by WHO (after the last wild-type case in 2011), but maintaining this status has been challenging.
Large, mobile and high-density population; reaching every child is logistically difficult.
Pockets of low immunisation coverage (urban slums, migrant communities, religious resistance in some areas).
Poor sanitation in some regions sustains faecal–oral transmission.
Vaccine-derived poliovirus (VDPV) can rarely emerge in under-immunised communities.
Cross-border transmission risk from neighbouring endemic countries (Pakistan, Afghanistan).
Hence continued vigilance and pulse campaigns are needed even after technical eradication.
Pulse Polio = mass OPV campaign on national immunisation days. OPV = oral live-attenuated polio vaccine giving mucosal + serum immunity. Slow eradication because of population size, sanitation gaps, vaccine refusal, and cross-border imports.
Challenges: population size, sanitation, refusal, imports.
Cross-check. Cross-check via three-layer prevention. (i) Source control: isolate cases, treat reservoirs. (ii) Transmission control: hygiene + vector control. (iii) Host protection: vaccination. WHO's smallpox eradication used all three; polio is approaching the same goal via OPV pulse drives.
Pulse Polio: oral live-vaccine mass drive; eradication slow due to logistics and sanitation gaps, but India achieved polio-free status in 2014.
Production workflow. Step 1: clone HBsAg gene into yeast expression vector with strong promoter (e.g. GAPDH, ADH1). Step 2: transform S. cerevisiae; select on auxotrophic marker. Step 3: ferment in bioreactor — yeast secretes HBsAg into medium. Step 4: harvest, purify by ultrafiltration + chromatography. Step 5: adsorb to aluminium hydroxide adjuvant. Step 6: vial, label, distribute. Total cycle: weeks vs months for live-virus vaccines.
Q 7.70
What are recombinant DNA vaccines? Give two examples of such vaccines. Discuss their advantages.
Concept used.Recombinant DNA vaccines are sub-unit vaccines made by inserting the gene encoding a pathogen's antigenic protein into a harmless host (yeast, bacterium, mammalian cell) which expresses and secretes the antigen. The purified antigen alone is used as the vaccine — without the pathogen itself.
Definition. Vaccines whose antigen is produced by recombinant-DNA technology rather than from cultured pathogens.
Steps in production.
Isolate the gene encoding the antigenic surface protein.
Clone it into a vector (plasmid).
Transform a host (e.g. yeast Saccharomyces cerevisiae).
Grow the host in bioreactors; the host expresses the antigen.
Purify the antigen and formulate as vaccine.
Two examples.
Hepatitis-B vaccine: HBsAg (Hepatitis B surface antigen) gene cloned into yeast Saccharomyces cerevisiae; yeast produces HBsAg, which is purified.
Human Papilloma Virus (HPV) vaccine (Cervarix, Gardasil): HPV L1 capsid protein produced in yeast / insect cells, self-assembles into virus-like particles.
Advantages.
Safety: no live pathogen, so cannot cause disease in the recipient.
Purity: a single defined antigen, free of contaminants from the original pathogen.
Scalability: yeast bioreactors produce huge quantities cheaply.
Stability: protein subunits are stable, easy to store and transport.
Designability: the antigen can be engineered for optimal immunogenicity (e.g. adjuvants, fusion proteins).
Useful when the pathogen is difficult to culture (Hepatitis B cannot be grown easily in lab).
Recombinant DNA vaccines use cloned antigen genes expressed in safe hosts. Examples: Hepatitis-B vaccine (HBsAg from yeast) and HPV vaccine (L1 from yeast). Advantages: safety, purity, scalability, stability, engineering flexibility.
AP
Aaditi Patel
Ph.D Molecular Biology, NCBS Bangalore
Verified Expert
Strategic angle. Define → workflow → examples → advantages, in that order.
Definition: vaccine antigen made via rDNA in a safe host.
Cross-check. Cross-check via retrovirus flow. Box 1 = viral DNA (the cDNA copy of viral RNA, produced by reverse transcriptase). Box 2 = new viral RNA + viral proteins (transcribed and translated from the integrated provirus). HIV ultimately destroys its CD4 T-cell host, which is the cause of AIDS-related immunosuppression.
Frequently Asked Questions on Human Health and Disease Class 12 Biology Exemplar Solutions
How many problems does the NCERT Exemplar Class 12 Biology Chapter 7 contain?
The Exemplar carries 70 problems split across 23 MCQ items, 16 Very Short Answer (VSA), 23 Short Answer (SA), and 8 Long Answer (LA) questions, every one of them answered in this Collegedunia PDF with full reasoning and an Expert's Solution.
Are the Class 12 Biology Chapter 7 Exemplar Solutions enough for NEET?
Yes for recall and phrasing, no for full coverage. The Exemplar locks the high-yield NEET phrases (CD4, gp120, metastasis, contact inhibition, sporozoite), but NEET aspirants should pair it with the previous year question set for assertion-reason items.
Is Human Health and Disease still part of the 2026-27 NCERT syllabus?
Yes. The 2026-27 NCERT retains the chapter in full, including AIDS, cancer and drug abuse. No sub-topic was dropped in the latest rationalisation, so every Exemplar problem on this page is examinable.
Which is the most asked Exemplar question type in Human Health and Disease?
Short Answer (SA) items dominate, 23 of the 70 questions are SA, and they map directly onto the 3-mark CBSE board pattern. Within SA, immunity and the Plasmodium life cycle are the two highest-frequency topics.
How is the Exemplar harder than the NCERT textbook for this chapter?
The textbook asks "define" and "name", the Exemplar asks "why" and "how". For example, NCERT asks the HIV target cell, Exemplar asks the receptor-ligand basis (gp120-CD4). The step-up is from recall to mechanism, which is the same step-up NEET expects.
Can I download the Exemplar Solutions PDF for free?
Yes, the full PDF is free to download from the card above. It covers all 70 problems, includes the Expert's Solution after every question, and is mapped to the 2026-27 NCERT chapter for Class 12 Biology Chapter 7.
What are the most common mistakes students make in Human Health and Disease?
Writing "WBCs" instead of "helper T-lymphocytes", confusing active and passive immunity, missing the haemozoin step in the Plasmodium life cycle, and treating benign tumours as if they could metastasise. All five mistakes are corrected inside the PDF.


































































































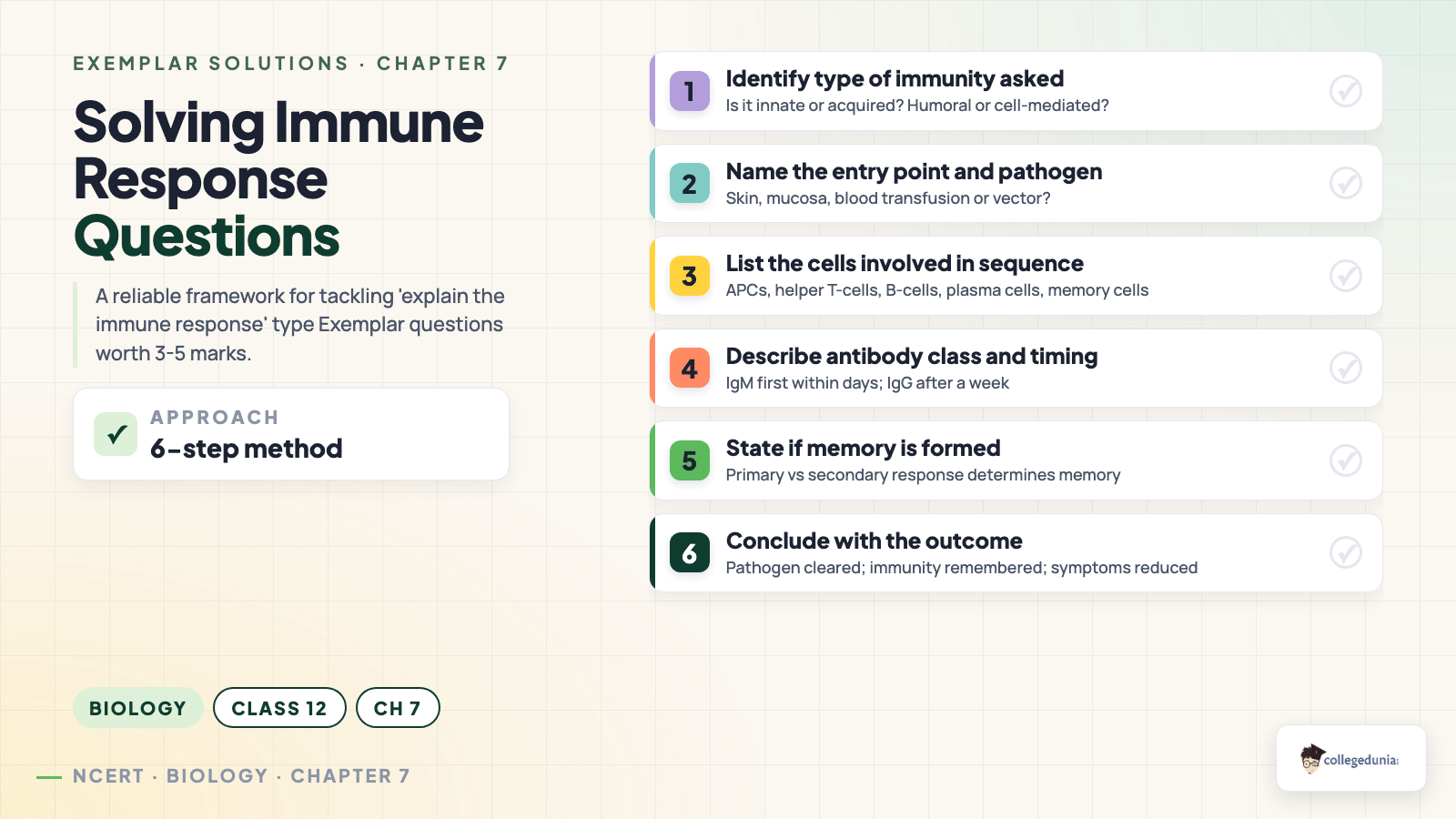
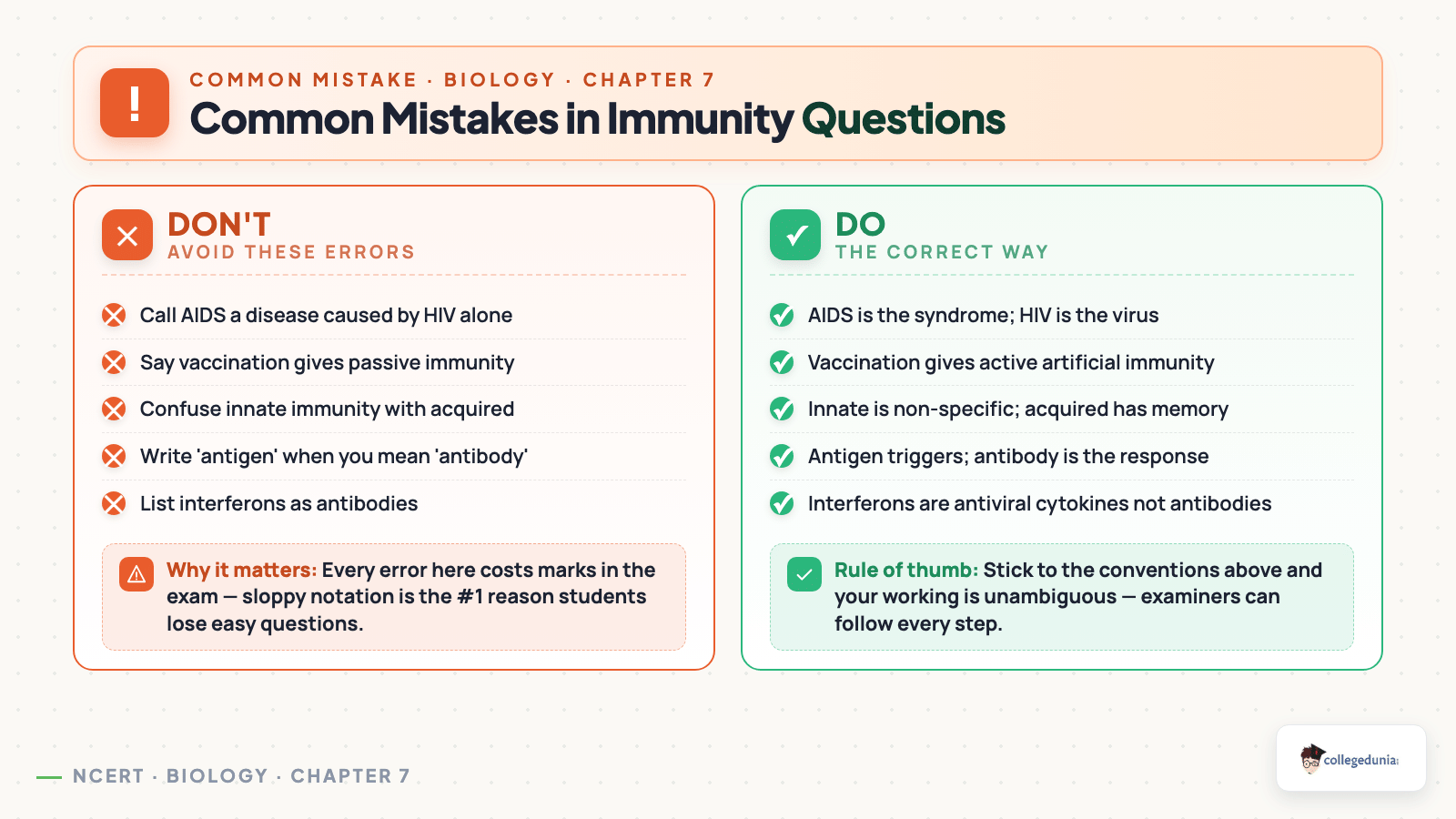
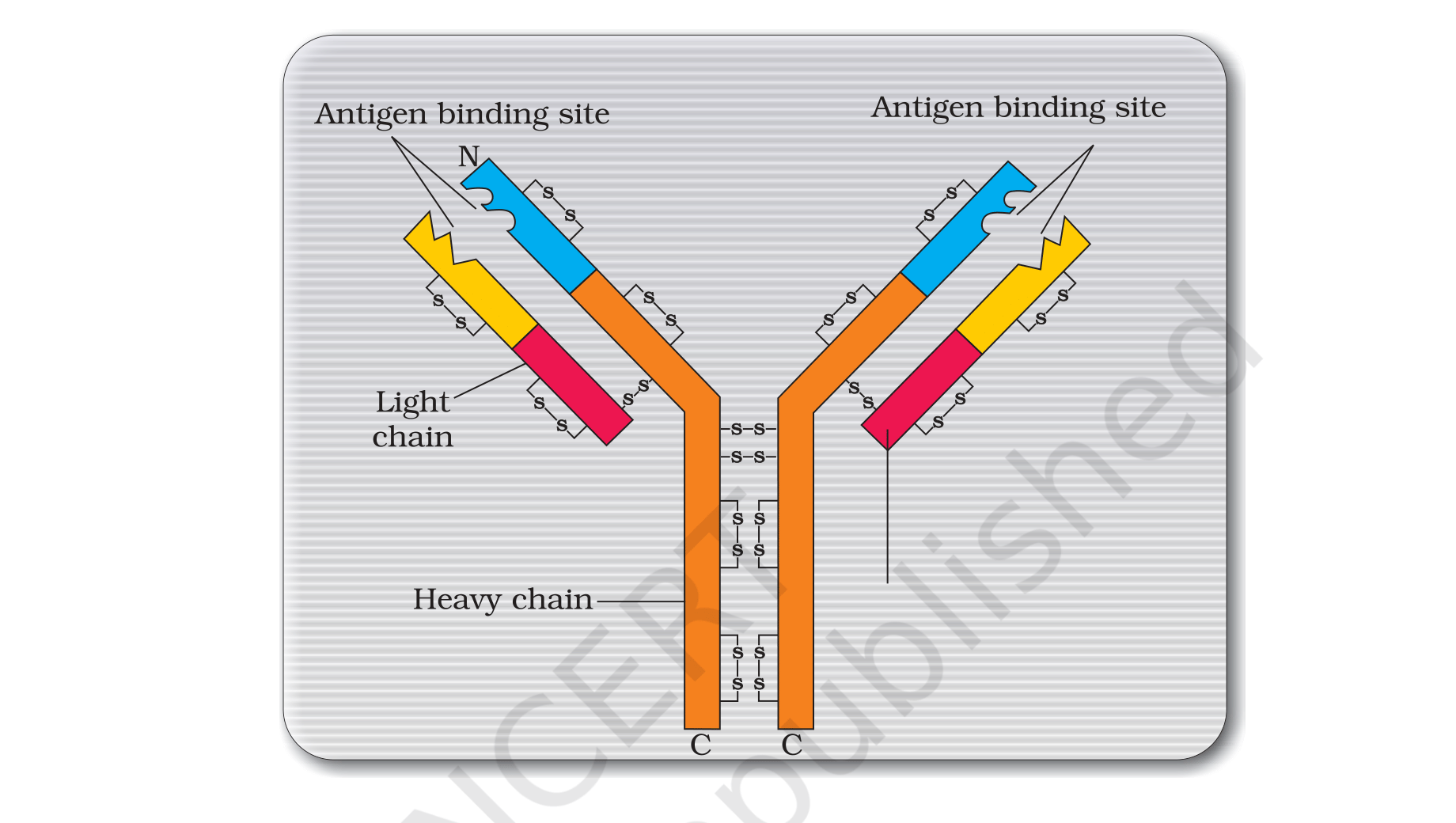
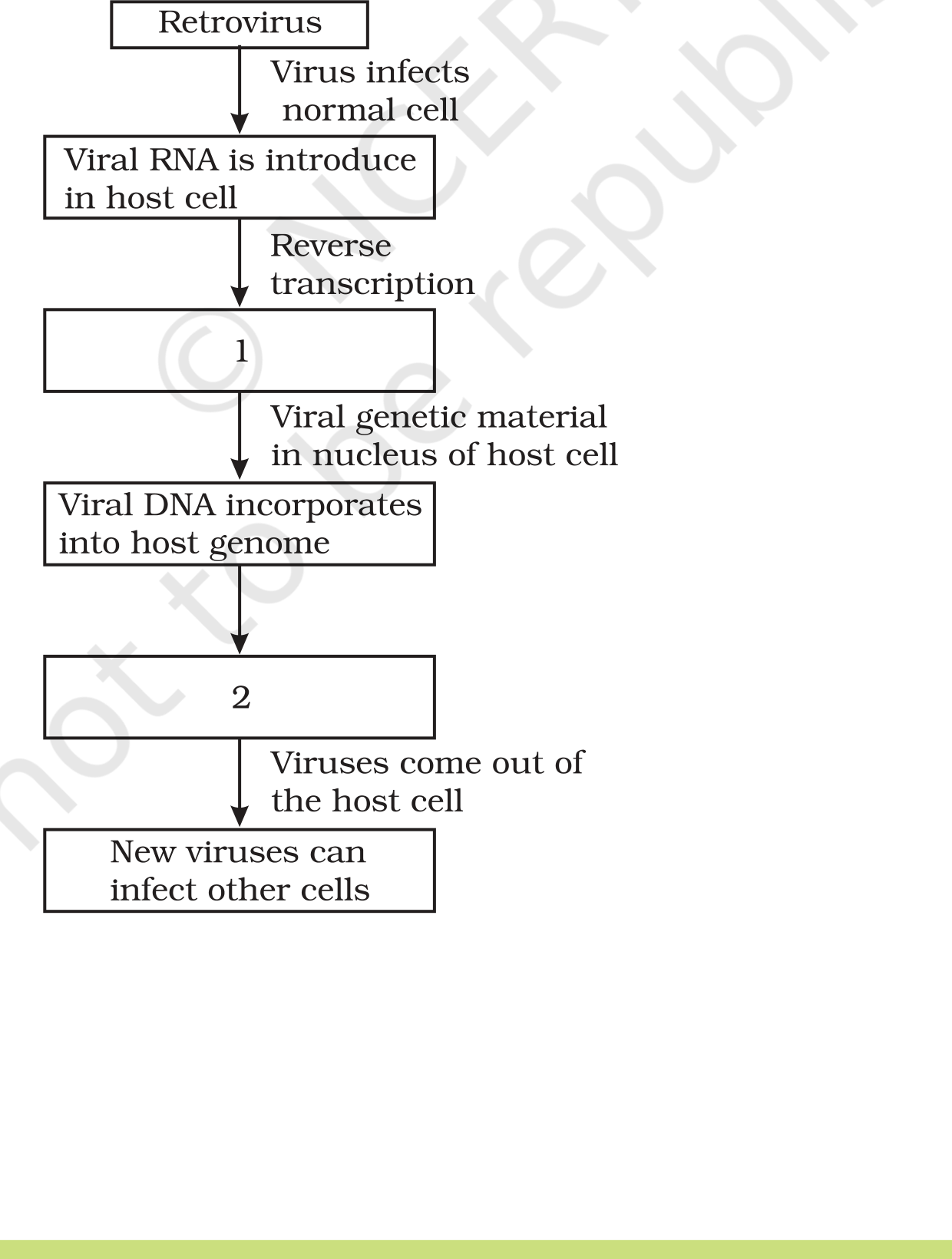


Comments